The PEDro Top 25 trials are ground-breaking trials that changed the way people are treated for a variety of conditions seen by physiotherapists and other healthcare professionals. Some of these trials set the stage for breakthroughs, some represent a paradigm shift, and all of them mark important milestones in the evolution of physiotherapy treatment.
About PEDro’s Top Trials list
PEDro’s Top trials began in 2014 to celebrate PEDro’s 15th anniversary. PEDro users were asked to nominate significant randomised controlled trials in physiotherapy published up to 2014. Nominations were judged by a panel of international physiotherapy trialists. This list became the PEDro Top 15 Trials. Since then, we have used this process to expand the list to the PEDro Top 20 Trials in 2019 by adding five new trials published from 2014-2019 to celebrate PEDro’s 20th anniversary. In 2024, five more trials published between 2019-2024 were added to form the PEDro Top 25 Trials to celebrate PEDro’s 25th anniversary.
We present the trials in order of publication, from the most recent to oldest.
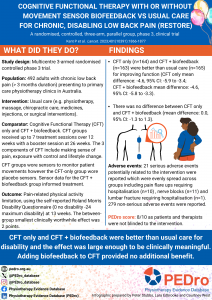
Cognitive functional therapy for chronic, disabling low back pain (RESTORE)
Kent P, Haines T, O'Sullivan P, Smith A, Campbell A, Schutze R, Attwell S, Caneiro JP, Laird R, O'Sullivan K, McGregor A, Hartvigsen J, Lee D-CA, Vickery A, Hancock M, on behalf of the RESTORE trial team
Lancet. 2023;401(10391):1866-1877. DOI: 10.1016/S0140-6736(23)00441-5.
Pelvic floor muscle training to treat urinary incontinence in older women
Dumoulin C, Morin M, Danieli C, Cacciari L, Mayrand MH, Tousignant M, Abrahamowicz M, Urinary Incontinence and Aging Study Group
JAMA Intern Med. 2020;180(10):1284-1293. DOI: 10.1001/jamainternmed.2020.2993.

Telerehabilitation for chronic respiratory disease
Telerehabilitation for chronic respiratory disease: a randomised controlled equivalence trial.
Cox NS, McDonald CF, Mahal A, Alison JA, Wootton R, Hill CJ, Zanaboni P, O'Halloran P, Bondarenko J, Macdonald H, Barker K, Crute H, Mellerick C, Wageck B, Boursinos H, Lahham A, Nichols A, Czupryn P, Corbett M, Handley E, Burge AT, Holland AE
Thorax. 2022;77(7):643-651. DOI: 10.1136/thoraxjnl-2021-216934.

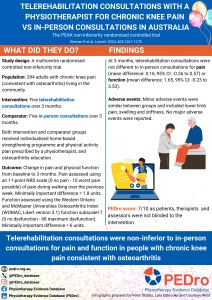
Telerehabilitation consultations with a physiotherapist for chronic knee pain (PEAK)
Hinman RS, Campbell PK, Kimp AJ, Russell T, Foster NE, Kasza J, Harris A, Bennell KL
Lancet. 2024; 403(10433):1267-78. DOI: 10.1016/S0140-6736(23)02630-2.
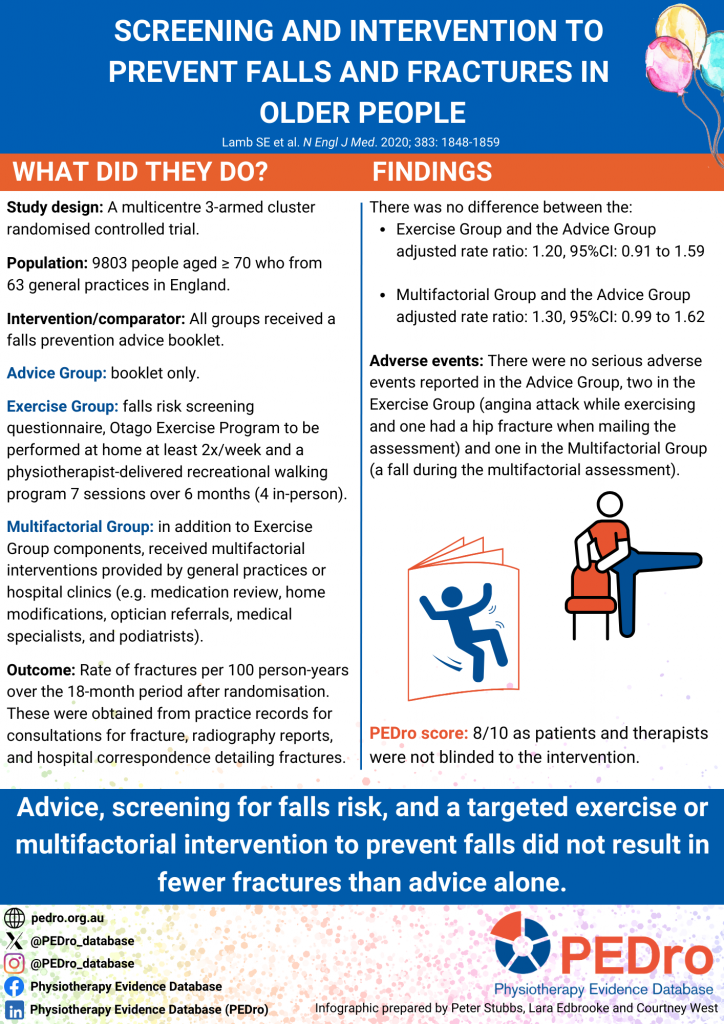
Screening and intervention to prevent falls and fractures in older people
Screening and intervention to prevent falls and fractures in older people.
Lamb SE, Bruce J, Hossain A, Ji C, Longo R, Lall R, Bojke C, Hulme C, Withers E, Finnegan S, Sheridan R, Willett K, Underwood M, for the Prevention of Fall Injury Trial Study Group
N Eng J Med. 2020; 383:1848-1859. DOI: 10.1056/NEJMoa2001500.
LIPPSMAck POP (Physiotherapy to prevent respiratory complications after abdominal surgery)
Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial
Boden I, Skinner EH, Browning L, Reeve J, Anderson L, Hill C, Robertson IK, Story D, Denehy L
BMJ 2018;360:j5916
Watch a video summarising the LIPPSMAck POP trial:
UK FASHIoN (Hip arthroscopy versus best conservative care for femoroacetabular impingement syndrome)
Hip arthroscopy versus best conservative care for the treatment of femoroacetabular impingement syndrome (UK FASHIoN): a multicentre randomised controlled trial
Griffin DR, Dickenson EJ, Wall PDH, Achana F, Donovan JL, Griffin J, Hobson R, Hutchinson CE, Jepson M, Parsons NR, Petrou S, Realpe A, Smith J, Foster NE, on behalf of the FASHIoN Study Group
Lancet 2018;391(10136):2225-35
Watch a video summarising the UK FASHIoN trial:
Listen to a podcast with Professor Damian Griffin and Professor Nadine Foster
HIHO (Inpatient rehabilitation versus a home-based program after total knee arthroplasty)
Effect of inpatient rehabilitation versus a monitored home-based program on mobility in patients with total knee arthroplasty: the HIHO randomized clinical trial
Buhagiar MA, Naylor JM, Harris IA, Xuan W, Kohler F, Wright R, Fortunato R
JAMA 2017;317(10):1037-46
Watch a video summarising the HIHO trial:
SARAH (Exercises to improve function of the rheumatoid hand)
Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial
Lamb SE, Williamson EM, Heine PJ, Adams J, Dosanjh S, Dritsaki M, Glover MJ, Lord J, McConkey C, Nichols V, Rahman A, Underwood M, Williams MA, on behalf of the Strengthening and Stretching for Rheumatoid Arthritis of the Hand Trial (SARAH) Trial Team
Lancet 2015;385(9966):421-9
Watch a video summarising the SARAH trial:
AVERT (Efficacy and safety of very early mobilisation within 24 h of stroke onset)
Efficacy and safety of very early mobilisation within 24 h of stroke onset (AVERT): a randomised controlled trial
The AVERT Trial Collaboration group
Lancet 2015;386(9988):46-55
Watch a video summarising the AVERT trial:
Exercise during hospital admission for an exacerbation of chronic respiratory disease
An early rehabilitation intervention to enhance recovery during hospital admission for an exacerbation of chronic respiratory disease: randomised controlled trial
Greening NJ, Williams JEA, Hussain SF, Harvey-Dunstan TC, Bankart MJ, Chaplin EJ, Vincent EE, Chimera R, Morgan MD, Singh SJ, Steiner MC
BMJ 2014;349:g4315
Watch a video summarising the Greening trial:
STarT Back (Stratified primary care management for low back pain)
Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial
Hill JC, Whitehurst DG, Lewis M, Bryan S, Dunn KM, Foster NE, Konstantinou K, Main CJ, Mason E, Somerville S, Sowden G, Vohora K, Hay EM
Lancet 2011;378(9802):1560-71
Watch a video summarising the STarT Back trial:
Read the transcript of an interview with Professor Jonathan Hill
Anne Moseley talked to Professor Jonathan Hill (Keele University, UK) whose trial evaluating stratified primary care management for low back pain is one of the 15 most significant trials in physiotherapy.
Anne: Explain what you did in the study
Jonathan: The STarT Back trial was designed to compare the clinical and cost effectiveness of stratified management of low back pain; allocating patients to targeted treatment pathways based on their screened prognostic risk category (low, medium, or high risk of poor outcome); with that of current best practice. The trial was carried out at the Arthritis Research UK Primary Care Centre, Keele University, UK, and was funded by a patient charity called Arthritis Research UK. The investigators recruited 851 adults with back pain between June 2007, and November 2008, from ten general practices in England. Patients were randomly assigned to stratified care (intervention group; 568) or current best practice of advice, exercise and manual therapy delivered by physiotherapists (control group; 283). The Roland and Morris Disability Questionnaire was used to measure whether the treatments helped relieve back pain and improved patients’ ability to function. The researchers also estimated the cost effectiveness of the two strategies in terms of quality adjusted life years (QALYS) and health-care costs.
Anne: What was the main finding?
Jonathan: At both 4 months and 12 months, patients in the intervention group showed a significant improvement in disability scores compared with patients in the control group. Additionally, at 12 months the intervention group were more likely to report reduced pain, fear, less depression, and better general health. Patients given the stratified care intervention were also significantly more likely to be satisfied with their treatment compared with current best care at 4 months, and took fewer days off work because of back pain over the 12 month study period. The stratified management intervention also resulted in a greater health benefit that was achieved at a lower average health-care cost.
Anne: Why do you think the study is important?
Jonathan: The STarT Back trial was the first study to test a stratified care approach for the management of back pain in primary care, and published in The Lancet, has been ground breaking in providing a simple and practical model for improving the effectiveness and costs of care compared to conventional pathways. Stratified care also enables clinicians to deliver more tailored services for patients with back pain and has challenged the existing one-size-fits-all and stepped care models suggested in current guidelines.
Anne: What lead you to do the study?
Jonathan: Around 9% of adults in the UK visit their general practitioner about back pain every year, but as many as 80% of these patients still report pain or disability a year after first consulting. Although trials have reported the benefits of a wide range of treatments such as exercise, manual therapies and cognitive behavioural approaches compared with standard care, a lack of evidence about which patients are likely to benefit from which interventions has reduced the efficiency of primary care management. The findings of this study represent an important advance in primary care management of back pain, and have important implications for commissioners and providers of services for back pain.
Anne: What studies are you conducting now?
Jonathan: Replication clinical trials of the STarT Back approach are currently being conducted in Seattle USA, led by Professor Dan Cherkin and separately by a Danish trial team led by Dr Lars Morsoe. The Keele team are currently undertaking research using a large clinical trial to test if a stratified care approach can be extended (using a combination of prognosis and clinical signs) for patients with sciatica presenting to primary care, including identifying which patients may need a fast-track pathway to receive a surgical opinion. A separate programme of research is also testing a new stratified care approach for patients with the 5 most common musculoskeletal conditions presenting to primary care including back, neck, shoulder, knee, and multi-site pain.
Anne: Jonathan, thank you for making such a valuable contribution to physiotherapy.
McKenzie method for acute low back pain
The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: a randomized controlled trial
Machado LAC, Maher CG, Herbert RD, Clare H, McAuley JH
BMC Medicine 2010;8(10):Epub
Watch a video summarising the Machado trial:
Listen to an interview with Dr Luciana Machado:
Early physical and occupational therapy in mechanically ventilated patients
Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial
Schweickert WD, Pohlman MC, Pohlman AS, Nigos C, Pawlik AJ, Esbrook CL, Spears L, Miller M, Franczyk M, Deprizio D, Schmidt GA, Bowman A, Barr R, McCallister KE, Hall JB, Kress JP
Lancet 2009;373(9678):1874-82
Watch a video summarising the Schweickert trial:
Read the transcript of an interview with Ms Amy Pawlik
Anne Moseley talked to Ms Amy Pawlik (University of Chicago Medicine, USA) whose trial evaluating early therapy in critically ill patients is one of the most significant trials in physiotherapy.
Anne: Could you explain what you did in the study
Amy: We divided patients who had recently been placed on a ventilator into two groups. One group underwent physical and occupational therapy when we would have typically seen them at that time, when the breathing tube was removed or a more permanent breathing tube was placed. The other group received physical and occupational therapy as early as possible after they had been placed on the ventilator. Patients in both groups received optimal nutrition, blood glucose control and a protocol that is used to reduce the usage of sedative medications. Both groups received physical and occupational therapy which included activities such as sitting in the chair, walking and participating in their own bathing and dressing. The difference between groups is that one group underwent physical and occupational therapy much earlier and while still requiring a ventilator and a breathing tube. At the time of the study, completing various out of bed activities such as standing, walking, and self-care tasks with patients on a ventilator with a breathing tube was not a common intervention.
Anne: What was the main finding?
Amy: Physical and occupational therapy were initiated much sooner in the early group; an average of 1.5 days after being placed on the ventilator versus 7 days with the standard group. The patients who received early physical and occupational therapy were able to come off the ventilator sooner, were better able to stand and walk independently when they were discharged from the hospital and experienced 50% fewer days of delirium, a state of confusion that is also associated with serious complications for patients who have been very ill. More patients were able to return immediately home after hospitalization as opposed to going to an alternate rehabilitation facility.
Anne: Why do you think your study is important?
Amy: There are many known long-lasting strength and cognition complications for patients who are in bed for days, weeks and even just hours. The study demonstrated that it is safe and possible to engage patients who need to be on a ventilator and while they are quite ill in aggressive physical and occupational therapy including out-of-bed activity very early in their hospital stay and that the patients who did so showed superior outcomes related to activities that are important to having a positive quality of life. It’s not enough to only help people recover medically from a serious illness; we need to do everything we can to ensure that, once a patient survives, he or she can return to the activities that allow the patient to be independent and enjoy life. This study helped change the way we manage patients with critical illness and this intervention is becoming the standard of care both in the United States and internationally.
Anne: What lead you to do the study?
Amy: Historically, patients with respiratory failure who were placed a ventilator were given medications to keep the patient calm, sedated, and immobile. We knew from earlier studies that when the sedative medications were not used, or used less, patients remained comfortable and were able to get off the ventilator sooner. However, often times these patients were still having chronic weakness and cognitive deficits which impair their day to day tasks. Our study built on this concept. We considered the possibility that, if the patients are safe and comfortable when awake on the ventilator and had improved outcomes, they might do even better if they did not remain confined to the bed but, instead, were engaged in activity to stimulate both the body and mind.
Anne: What studies are you conducting now?
Amy: Our study followed the patients until they left the hospital. But, it did not tell us what happened in the long run. We are replicating the original study but following the patients after they leave the hospital to see if the improvements we had noted in the first study hold up over time.
Anne: Amy, thank you for making such a valuable contribution to physiotherapy.
Diclofenac or spinal manipulation for acute low back pain
Assessment of diclofenac or spinal manipulative therapy, or both, in addition to recommended first-line treatment for acute low back pain: a randomised controlled trial
Hancock MJ, Maher CG, Latimer J, McLachlan AJ, Cooper CW, Day RO, Spindler MF, McAuley JH
Lancet 2007;370(9599):1638-43
Watch a video summarising the Hancock trial:
Listen to an interview with Professor Mark Hancock:
Mobilisation and exercise, injection, or wait and see for tennis elbow
Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial
Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B
BMJ 2006;333(7575):939-44
Watch a video summarising the Bisset trial:
Listen to an interview with Dr Leanne Bisset and Professor Bill Vicenzino:
EXCITE (Effect of constraint-induced movement therapy after stroke)
Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: the EXCITE randomized clinical trial
Wolf SL, Winstein CJ, Miller JP, Taub E, Uswatte G, Morris D, Giuliani C, Light KE, Nichols-Larsen D, for the EXCITE Investigators
JAMA 2006;296(17):2095-104
Watch a video summarising the EXCITE trial:
Listen to an interview with Professor Steven Wolf:
FOPANU (Frail Older People – Activity and Nutrition study in Umeå)
High-intensity functional exercise program and protein-enriched energy supplement for older persons dependent in activities of daily living: a randomised controlled trial
Rosendahl E, Lindelof N, Littbrand H, Yifter-Lindgren E, Lundin-Olsson L, Haglin L, Gustafson Y, Nyberg L
Australian Journal of Physiotherapy 2006;52(2):105-13
Watch a video summarising the FOPANU trial:
Read the transcript of an interview with Dr Erik Rosendahl
Anne Moseley talked to Dr Erik Rosendahl (Umeå University, Sweden) whose trial evaluating exercise for older persons is one of the most significant trials in physiotherapy.
Anne: Could you explain what you did in the study
Erik: The Frail Older People - Activity and Nutrition Study in Umeå (the FOPANU Study) evaluated a high-intensity functional exercise program in older people living in residential care facilities.
Anne: What was the main finding?
Erik: In the FOPANU Study it was demonstrated that the exercise program had important positive effects on, for example, gait, lower-limb strength, balance, and dependency in activities of daily living when compared to a control activity program. In addition, the exercise program used in the trial (the High-Intensity Functional Exercise Program, the HIFE Program) was shown to be as applicable for people with dementia as for people without.
Anne: Why do you think your study is important?
Erik: The FOPANU Study was the first trial evaluating a high-intensity functional exercise program in older people with severe cognitive and physically impairment including those with dementia. Among the 191 participants, all living in residential care facilities; mean age was 85 years, half had a dementia diagnosis and two thirds were not able to rise up from a chair independently. Rehabilitation for older people with impairments is an important and expanding working field in clinical practice and research for physiotherapists, especially considering that the world population is aging rapidly. Today around 35 million people have dementia and this number is estimated to double by 2030 and more than triple by 2050. According to the World Health Organisation (WHO), dementia is defined as the leading course of disability and dependency among older people and should be considered as a public health priority.
Anne: What lead you to do the study?
Erik: Nina Lindelöf, and Håkan Littbrand and I developed the HIFE Program based on the experiences from clinical work and a previous study. We wanted to develop an exercise program that could easily be implemented due to well-described exercises, standardized instructions, and portable exercise equipment. We knew from the literature that high intensity and functional exercises were important for the exercise effect and wanted to evaluate if it was feasible and effective also for older people with severe cognitive and physically impairments.
Anne: What studies are you conducting now?
Erik: One example is the Umeå Dementia and Exercise (UMDEX) Study. In the UMDEX Study, we are evaluating the effect of the HIFE Program among 186 older people with dementia on several outcomes. Hopefully, the first results from this study will be published in the beginning of next year.
Anne: Erik, thank you for making such a valuable contribution to physiotherapy.
Exercises to prevent lower limb injuries in youth sports
Exercises to prevent lower limb injuries in youth sports: cluster randomised controlled trial
Olsen OE, Myklebust G, Engebretsen L, Holme I, Bahr R
BMJ 2005;330(7489):449-55
Watch a video summarising the Olsen trial:
Read the transcript of an interview with Professor Odd-Egil Olsen
Anne Moseley talked to Professor Odd-Egil Olsen (UiT Norges Arktiske Universitet, Norway) whose trial evaluating exercise to prevent sporting injuries is one of the 15 most significant trials in physiotherapy.
Anne: Explain what you did in the study
Odd-Egil: In the study we investigated the effect of a structured warm-up program designed to reduce the incidence of knee and ankle injuries in young people participating in sports. We followed 120 team handball clubs and registered all injuries during one 8-month season. At the start of the league season, the clubs in the intervention group received a program of warm-up exercises to prevent injuries, while the clubs in control group where doing their training as usual.
Anne: What was the main finding?
Odd-Egil: The main finding was that a structured warm-up program with exercises to improve awareness and knee and ankle control during landing and pivoting movements reduces injuries to the lower limb in youth team handball.
Anne: Why do you think the study is important?
Odd-Egil: The randomised controlled trial is important because it shows that the incidence of knee and ankle injuries can be reduced by at least 50%. Preventive training should therefore be routine and a natural part of youth sports training programs. Also, programs focusing on technique and balance training should be implemented in players as young as 10-12 years. It seems reasonable to assume that the prevention program used in the study also could be modified to be used in other similar sports, and that question should lead to future research.
Anne: What lead you to do the study?
Odd-Egil: Participation in sports entails a risk of injury, and sports injuries constitute 10-19% of all acute injuries treated in emergency departments, with injuries to the knee and ankle the most common types. The risk of serious knee injuries, such as injuries to the anterior cruciate ligament, is high among adolescents playing pivoting sports such as football, basketball, or team handball. Previously studies showing that it may be possible to reduce the incidence of knee and ankle injuries among young people have been small and mainly non-randomised, with significant methodological limitations. Therefore, we initiated the randomised controlled trial with high enough sample size to investigate the effect of a prevention program.
Anne: What studies are you conducting now?
Odd-Egil: One of the coauthors of the paper, Associate Professor Grethe Myklebust, has followed the anterior cruciate ligament injury incidence in female handball for 15 years, and received important lessons learned from the Norwegian anterior cruciate ligament prevention study. Furthermore, she along with Dr Kathrin Steffen and Professor Roald Bahr from the Oslo Sports Trauma Research Center have been the driving force behind the free app "Get Set - Train Smarter". Get Set provides injury prevention exercises, which were created for the occasion of the 2014 Youth Olympic Games.
Anne: Odd-Egil, thank you for making such a valuable contribution to physiotherapy.
Additional task-related practice after stroke
Additional task-related practice improves mobility and upper limb function early after stroke: a randomised controlled trial
Blennerhassett J, Dite W
Australian Journal of Physiotherapy 2004;50(4):219-24
Watch a video summarising the Blennerhassett & Dite trial:
Listen to an interview with Dr Jannette Blennerhassett and Dr Wayne Dite:
Extracorporeal shock wave therapy for plantar fasciitis
Ultrasound-guided extracorporeal shock wave therapy for plantar fasciitis. A randomized controlled trial
Buchbinder R, Ptasznik R, Gordon J, Buchanan J, Prabaharan V, Forbes A
JAMA 2002;288(11):1364-72
Watch a video summarising the Buchbinder trial:
Read the transcript of an interview with Professor Rachelle Buchbinder
Anne Moseley talked to Professor Rachelle Buchbinder (Monash University, Australia) whose trial evaluating extracorporeal shock wave therapy for plantar fasciitis is one of the most significant trials in physiotherapy.
Anne: Explain what you did in the study
Rachelle: The aim of our study was to determine whether extracorporeal shock wave therapy is effective for people with heel pain due to plantar fasciitis. We randomised 166 participants to receive either this therapy given weekly for three weeks or an identical placebo. Neither the investigators nor the participants knew which treatment was received. We measured pain and function including walking ability at baseline, at 6 and 12 weeks.
Anne: What was the main finding?
Rachelle: We found that both treatment groups improved over time but there was no statistical or clinically important difference in the degree of improvement between groups for any of the measured outcomes.
Anne: Why do you think the study is important?
Rachelle: The study is important because we found that this treatment has no intrinsic therapeutic value in the treatment of this common condition and it has led to a change in practice.
Anne: What led you to do the study?
Rachelle: Extracorporeal shock wave therapy was becoming an increasingly used treatment for plantar fasciitis as well as other regional conditions such as lateral epicondylitis (tennis elbow). However there was limited evidence from high quality trials to support its use.
Anne: What studies are you conducting now?
Rachelle: We performed a similar trial of extracorporeal shock wave therapy for lateral epicondylitis which was also unable to demonstrate any benefit of the therapy over an identical sham. We are continuing to perform trials to assess the efficacy and safety of various interventions for regional conditions including shoulder, elbow and foot pain as well as osteoarthritis. Currently we are performing a three-arm placebo-controlled trial to determine the efficacy and safety of platelet-rich plasma injection and glucocorticoid injection for lateral epicondylitis.
Pelvic floor exercise for stress incontinence
Single blind, randomised controlled trial of pelvic floor exercises, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence in women
Bø K, Talseth T, Holme I
BMJ 1999;318(7182):487-93
Watch a video summarising the Bø trial:
Read the transcript of an interview with Professor Kari Bø
Anne Moseley talked to Professor Kari Bø (Norges Idrettshøgskole, Norway) whose trial evaluating pelvic floor muscle training for urinary incontinence is one of the 15 most significant trials in physiotherapy.
Anne: Explain what you did in the study
Kari: This was a four arm assessor blind randomised controlled trial comparing the effect of a 6 month intervention with either pelvic floor muscle training, use of vaginal weighted cones, electrical stimulation or untreated control. 8 physiotherapists and 5 urologists/gynaecologists conducted the study. The urologists/gynaecologists who evaluated the main outcome were blinded to group allocation. All interventions followed best practice for that method (for example, use of best practice for electrical stimulation parameters).
Anne: What was the main finding?
Kari: The main finding was that only pelvic floor muscle training was effective in improving pelvic floor muscle strength and reducing urinary incontinence in women with stress urinary incontinence (measured by pad test with standardised bladder volume). The women in the pelvic floor muscle training group were also more satisfied and wanted less further treatment. There was no discomfort or side effects in the pelvic floor muscle training group.
Anne: Why do you think the study is important?
Kari: It is important because it was shown in a blinded randomised controlled trial that pelvic floor muscle training was more effective than other methods that required more expensive equipment. Pelvic floor muscle training was the only method that showed an effect over that of an untreated control. The effect size based on the pad test was good.
Anne: What lead you to do the study?
Kari: When I published my first trial on pelvic floor muscle training in 1990 it was one of very few trials in the world on this topic. I compared two different approaches to pelvic floor muscle training and found that more intensive training with close follow up once a week was more effective than a less intensive approach. After that there was a boom of studies (usually non-randomised and pre-post-test designs) emerging which had direct influence on clinical practice. Methods like electrical stimulation and vaginal weighted cones were marketed as effective (there was more money behind these than simple strength training which was not marketed at all) although pelvic floor muscle training in my opinion had a much stronger theoretical rationale. A four arm randomised controlled trial comparing all these methods with an untreated control was therefore necessary.
Anne: What studies are you conducting now?
Kari: We have just finished a cohort study following 300 first time pregnant women with measurement of pelvic floor muscle function using transperineal ultrasound and vaginal pressure measurements plus a lot of other clinical assessments and questionnaires. The women have been assessed at gestational week 21 and 37 and 6 weeks, 6 months and 12 months postpartum. In addition we have finished an assessor blinded randomised controlled trial starting 6 weeks postpartum and lasting for 4 months. We have measured different outcomes, with urinary incontinence being the primary outcome. We also have data on diastasis recti abdominis, pelvic organ prolapse, pelvic pain, sexual dysfunction, pelvic girdle pain, low back pain and physical activity level. I am also supervising a physiotherapist at the University of Lisboa, Patricia Mota, who has submitted her PhD thesis on diastasis recti abdominis and have a new PhD student in Iceland, Thorbjørgur Sigurdardottir, working on a project in sports women and urinary incontinence and a randomised controlled trial on pelvic floor muscle training to treat faecal incontinence. In addition, I have 3 PhD students in gynaecology and 2 physiotherapists. I appreciate very much the collaboration with medical professionals. Sometimes we are not interested in the same question (which is good) and sometimes we disagree, but I am sure this collaboration makes both professions better. We must talk the same language and be in the same room to do the best for our patients.
Anne: Kari, thank you for making such a valuable contribution to physiotherapy.
Traction for non-specific low back pain
Efficacy of traction for non-specific low back pain: a randomised clinical trial
Beurskens AJ, de Vet HC, Koke AJ, Lindeman E, Regtop W, van der Heijden GJ, Knipschild PG
Lancet 1995;346(8990):1596-1600
Watch a video summarising the Beurskens trial:
Read the transcript of an interview with Professor Sandra Beurskens and Professor Riekie de Vet
Anne Moseley talked to Professor Sandra Beurskens (Zuyd University of Applied Sciences and Maastricht University, Netherlands) and Professor Riekie de Vet (VU University Medical Center, Netherlands) whose trial evaluating traction for low back pain is one of the 15 most significant trials in physiotherapy.
Anne: Could you explain what you did in the study
Sandra and Riekie: We compared traction to sham traction in people with low back pain (n=151). Two different doses of traction were used – 35-50% (high dose) and less than 20% (low dose or sham) of the patient’s body weight using a split table. The patients and assessors were blinded for the assigned treatment. It was quite a challenge to develop the sham traction, but we thought this was a very important aspect of the study. Comparing traction to a sham (or placebo) increased the rigor of the study. The sham traction involved the patient wearing a special brace around the iliac crest. The patients were told that they only had to feel a little pulling from the brace while receiving a very small amount of traction (less than 20% of body weight). The brace became tighter in the back during treatment. This was experienced as if traction were exerted.
Anne: What was the main finding?
Sandra and Riekie: There was no difference between the traction and sham groups for any of the outcome measures. We used a number of outcome measures. The main outcome was the global impression of perceived effect and the Patient Specific Complaint scale (which is comparable to the Patient Specific Complaints scale). Other outcomes included pain, range of motion and disability. Our data did not support the claim that traction is effective for patients with low back pain.
Anne: Why do you think your study is important?
Sandra and Riekie: We set the trial up in the early 1990’s. At that time traction was a commonly used treatment for low back pain. Traction is a very passive treatment for the patient. Earlier trials on traction did not allow clear conclusions due to methodological flaws. We wanted to work out if it was worthwhile.
Anne: What lead you to do the study?
Sandra and Riekie: When we were setting up the trial it was a commonly held belief that it was not possible to use a randomised controlled trial to evaluate physiotherapy intervention because treatment was so tailored to individual patients. We wanted to conduct a robust randomised controlled trial because it was important for the profession to start rigorously evaluating physiotherapy treatments. We succeeded in performing a high quality trial that was published in The Lancet.
Anne: What studies are you conducting now?
Sandra: This was the only study I conducted on traction for low back pain. Other trails were about mental practice and mirror therapy. At present my work focuses on goal orientated measurement in daily practice, in musculoskeletal and other health areas, for physiotherapists and interdisciplinary (occupational therapy, nurses, speech therapists and physicians). A component of my work is the implementation of outcome measurement in clinical practice.
Riekie: I went on to be involved in a number of studies evaluating the effects of a number of physiotherapy interventions, including laser, graded activity and high-intensity interventions for low back pain as well as other musculoskeletal conditions (for example, neck or shoulder pain). Outcome measurement is also a focus of my current research.
Anne: Sandra and Riekie, thank you for making such a valuable contribution to physiotherapy.
Evaluation of a fitness programme for patients with chronic low back pain
Randomised controlled trial for evaluation of fitness programme for patients with chronic low back pain
Frost H, Klaber Moffett JA, Moser JS, Fairbank JC
BMJ 1995;310(6973):151-4
Watch a video summarising the Frost trial:
Read the transcript of an interview with Dr Helen Frost
Anne Moseley talked to Dr Helen Frost (Scottish Collaboration for Public Health Research and Policy, UK) whose trial evaluating fitness training for chronic low back pain is one of the 15 most significant trials in physiotherapy.
Anne: Could you explain what you did in the study
Helen: The study evaluated a fitness program, designed to encourage people with chronic low back pain to become more physically active. People with chronic low back pain were randomised to 2 groups – both groups attended a back education program (back school) and were advised to exercise at home. In addition, one group also attended a progressive fitness program, twice a week for 4 weeks.
Anne: What was the main finding?
Helen: People who attended the fitness program reported less pain and disability than those that were advised to exercise on their own at home, at 6 months and 2 years after the intervention. They were able to walk further and faster and reported more confidence in their ability to carry out normal activities of daily living.
Anne: Why do you think your study is important?
Helen: At the time this study was carried out people with back pain were generally being treated very conservatively, sometimes even with bed rest but mostly on a one-to-one basis with passive treatment. So the fitness program aimed to give people confidence to exercise and take a more active approach to their back pain. Whilst it wasn't a new idea, as exercise has always been the root of the physiotherapy profession, in a hospital setting it was one of the first programs to be evaluated in a randomised controlled trial. It was a small single-centre study that led to other bigger multi-centre trials of physiotherapy intervention.
Anne: What lead you to do the study?
Helen: Research supported the need to change the approach to managing back pain and there was evidence to suggest that back pain should be treated more actively, yet most people with back pain didn't know where to start and were often afraid to exercise. The back fitness program was developed as a "stepping stone" to help people overcome their fear of exercise. As it was a new service developed in a hospital setting, it was important to evaluate it.
Anne: What studies are you conducting now?
Helen: I am not carrying out any studies at the moment but I am very interested in developing research ideas aimed at encouraging older people to be more physically active and less sedentary.
Anne: Helen, thank you for making such a valuable contribution to physiotherapy.
Physiotherapy for Bell's palsy
Physiotherapy for Bell's palsy
Mosforth J, Taverner D
British Medical Journal 1958;2(5097):675-7
This 1958 trial is significant because it was one of the first trials evaluating a physiotherapy treatment. It found no significant benefit from the use of galvanic stimulation for Bell's palsy.
Watch a video summarising the Mosforth & Taverner trial:
Read the transcript of an interview with Mr Lázaro Teixeira, who included this trial in his Cochrane review
Bruno Saragiotto talked to Mr Lázaro Teixeira who included one of the 15 most significant trails in physiotherapy, the 1958 trial evaluating physiotherapy for Bell’s palsy, in his Cochrane review.
Bruno: Could you explain what Mosforth and Taverner did in their study?
Lázaro: In 1958, Mosforth and Taverner tried to answer one of the oldest questions in neuromusculoskeletal physiotherapy - if the addition of electrical stimulation is worthwhile and if it helps the recovery of a peripheral neural lesion, in this case idiopathic facial palsy. They designed a randomised controlled trial to compare two groups of participants with acute cases of facial palsy. The study enrolled 86 people. The clinical outcomes of 44 people in the group that received auto-massage of the face, infrared radiation and electrical stimulation (interrupted galvanism) were compared to the results of the group (42 people) that received auto-massage alone. The physiotherapeutic treatment was continued until recovery, and then the participants were followed up 6 months and 1 year after their first visit. The outcomes were: electrical examination, grade of paralysis, time to begin improvement, time to complete recovery, and side effects.
Bruno: What was the main finding?
Lázaro: The study didn't find significant differences between the 2 treatment groups for any outcomes after 6 months or 1 year.
Bruno: Why do you think the study is important?
Lázaro: This study evaluated physiotherapy for facial palsy and it was one of the first randomised controlled trials for any condition in the field of physiotherapy. Despite the age of the trial, it is still one of the best designed studies to evaluate treatments for idiopathic facial palsy. Mosforth and Taverner followed participants for 1 year. Even today, it is difficult to find studies in this area with long term follow ups. More than 55 years ago, Mosforth and Taverner concluded electrical stimulation is not recommended for the treatment of facial palsy and questioned its cost-effectiveness. This finding has been supported by subsequent studies.
Bruno: Lázaro, thank you for telling us about the Mosforth and Taverner trial.