Return to all evidence summaries
Cardiothoracics
Cardiothoracics includes, but is not restricted to, papers evaluating acute and rehabilitation cardiothoracic interventions or fitness training on those with conditions affecting the cardiothoracic system. This subdiscipline does not include studies of general fitness training among patient populations. Studies of general fitness training for healthy populations are not indexed on PEDro.
The most recently synthesised review is at the top of the list.
- Inspiratory muscle training to reduce risk of pulmonary complications after coronary artery bypass grafting
- Multimodal prehabilitation and postoperative outcomes in upper abdominal surgery
- Preoperative respiratory muscle training reduces the risk of pulmonary complications and the length of hospital stay after cardiac surgery
- Exercise‐based cardiac rehabilitation for adults with heart failure
- Exercise-based rehabilitation programmes for pulmonary hypertension
- Physical activity and exercise training in cystic fibrosis
- Rehabilitation to enable recovery from COVID-19
- Efficacy of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery
- Effectiveness of aerobic exercise on smoking cessation in adults
- Advanced telehealth technology improves home-based exercise therapy for people with stable chronic obstructive pulmonary disease
- Pulmonary rehabilitation can improve the functional capacity and quality of life for pneumoconiosis patients
- Early rehabilitation reduces the likelihood of developing intensive care unit-acquired weakness
- How does exercise treatment compare with antihypertensive medications?
- Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema
- Exercise therapy for functional capacity in chronic diseases
- Efficacy of different types of exercise-based cardiac rehabilitation on coronary heart disease
- Cardiac rehabilitation and physical activity
- Supervised exercise therapy versus home-based exercise therapy versus walking advice for intermittent claudication
- Short-term efficacy of minimally invasive treatments for adult obstructive sleep apnea
- Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease
- Exercise-based cardiac rehabilitation in heart transplant recipients
- Implementing resistance training in the rehabilitation of coronary heart disease
- Exercise training alone or with the addition of activity counseling improves physical activity levels in COPD
- Effect of exercise training on sleep apnea
- The effect of early rehabilitation on therapeutic outcomes in ICU patients on mechanical ventilation
Inspiratory muscle training to reduce risk of pulmonary complications after coronary artery bypass grafting
Coronary artery bypass grafting (CABG) is a common surgical treatment for many types of cardiovascular and coronary heart disease. However, people undergoing CABG surgery have a high-risk of developing post-operative pulmonary complications (PPCs). This systematic review aimed to synthesise and appraise the quality of evidence for the use of inspiratory muscle training (IMT), either pre- or post-operatively, for patients treated with CABG.
Five databases were searched for published studies with no language restrictions from inception to March 2023. Eligible studies were randomised controlled trials (RCTs) that used IMT to treat adult patients, >18 years of age, either prior to or following CABG surgery. The comparator was usual care, sham IMT or physiotherapy. Included trials reported at least one post-operative pulmonary complications (pneumonia, atelectasis, or pleural effusion).
The primary outcome was PPCs, measured by rates of pneumonia, atelectasis and pleural effusion. Secondary outcomes were respiratory function (including maximal inspiratory and expiratory pressures), hospital length of stay and exercise capacity. Adverse events were not assessed in the review. Study selection, data extraction and assessment of methodological quality, using the Cochrane Collaboration Risk of Bias tool (version 2), were performed by two authors independently. Evidence quality was assessed for the primary outcome only using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system. Meta-analyses using random effects models were used if statistical heterogeneity was >50%. Results were reported as relative risks (RR) or mean differences (MDs), with associated 95% confidence intervals (CIs). Subgroup analysis compared the effects of pre-operative and post-operative IMT on maximal inspiratory pressure (MIP).
Eight trials with 755 participants (range 20-276) were included in the systematic review and meta-analysis. Trials compared IMT to usual care (5 trials), IMT to physiotherapy (2 trials) and IMT to sham IMT (1 trial). The intervention was delivered in the pre-operative period in four trials (n=621). Interventions varied with IMT being performed 1-2 times a day at an intensity of 30-60% maximal inspiratory pressure. Intervention duration ranged from 3 days to 4 weeks. Risk of bias was rated as ‘low’ in 2 trials, of ‘some concerns’ in 3 trials and ‘high’ in 3 trials. High risk of bias was attributable to lack of allocation concealment (2 trials); and lack of participant or assessor blinding (4 trials).
Compared to usual care, sham IMT or physiotherapy treatments, IMT reduced the risk of PPCs – pneumonia (RR = 0.39, 95% CI 0.25 to 0.62, p < 0.0001, n = 755, 8 trials, I2 = 0%, moderate quality evidence); and atelectasis (RR = 0.43, 95% CI 0.27 to 0.67, p=0.0002, n = 244, 6 trials, I2 = 0%, low quality evidence); but not pleural effusion (RR = 1.09, 95% CI 0.62 to 1.93, p=0.76, n = 244, 6 trials, I2 = 18%, very low quality evidence). No between group differences were found for exercise capacity, however the intervention group had significantly improved respiratory function and reduced hospital length of stay. Subgroup analysis showed preoperative IMT led to greater improvements in MIP than postoperative IMT (MD = 16.55 cmH₂O, 95% CI 13.86 to 19.24, p < 0.00001, n = 624, 4 trials vs. MD = 8.99 cmH₂O, 95% CI 2.39 to 15.60, p = 0.008, n = 114, 3 trials).
Evidence from moderate to low quality trials suggests IMT, compared to usual care, sham IMT or physiotherapy treatments, reduces the risk of pneumonia and atelectasis in patients following CABG, and shortens hospital stay.
Xiang Y, Zhao Q, Luo T, Zeng L. Inspiratory muscle training to reduce risk of pulmonary complications after coronary artery bypass grafting: a systematic review and meta-analysis. Front Cardiovasc Med. 2023 Jul 24;10:1223619. doi: 10.3389/fcvm.2023.1223619

Multimodal prehabilitation and postoperative outcomes in upper abdominal surgery
Over 4 in 10 adults over the age of 60 will undergo abdominal surgery at some point in their life, 30% of which will experience post operative complications. Prehabilitation aims to reduce recovery time and can also improve eligibility for patients who would otherwise not qualify for surgery. This systematic review investigated the effect of prehabilitation on patients with sarcopenia or frailty undergoing elective upper abdominal surgery on post operative outcomes compared to those not undergoing prehabilitation.
Four databases (MEDLINE, Embase, CINAHL and Cochrane CENTRAL) were searched for randomised controlled trials from the year 2000 onwards with no language restriction. Eligible studies included adults with sarcopenia or frailty undergoing upper abdominal surgery; primary outcomes were postoperative pulmonary complications (PPCs) and all cause complications (measured by using log-odds ratios), secondary outcomes were functional capacity, length of hospital stay (LOS), intensive care unit (ICU) stay (measured by mean differences). Prehabilitation interventions were physical therapy, nutritional therapy, psychosocial, anaemia-related, respiratory therapy compared to no prehabilitation. Two raters independently extracted data and disagreements were resolved by consensus. The review was processed in accordance with PRISMA and AMSTAR-2 guidelines and the risk of bias of RCTs was assessed using the Joanna Briggs Institute (JBI) 13-point critical appraisal checklist. Meta-analysis was performed using random effect model, heterogeneity was performed using I2 and sensitivity analysis was also performed. Heterogeneity was evaluated using a random effects model I-square, and sensitivity analysis and meta-analysis were performed.
The review included 10 trials (1,503 participants). Studies were conducted in Spain (n=2), United Kingdom (n=2), Canada (n=2), Netherlands (n=1), Brazil (n=1), Australia and New Zealand (n=1) and Australia (n=1). Prehabilitation ranged between 8 days to 6 weeks, and modes of prehabilitation included exercise training only (n=4), combined exercise and inspiratory muscle training (n=3), combined exercise training and nutrition support (n=2) and anaemia treatment only (n=1). Study quality ranged between 8 and 13 on the JBI critical appraisal checklist.
Compared to no prehabilitation, prehabilitation reduced the odds of developing PPCs (OR -0.96, 95% CI -1.38 to -0.54, I2 = 0%)(5 trials, 674 participants) and reduced all cause complications (OR -0.21, 95% CI -0.475 to 0.055, I2 = 41.06%)(9 trials, 1336 participants). Prehabilitation overall did not reduce hospital LOS (SMD -0.48, 95% CI -1.34 to 0.38, I2 = 39.6%) (10 trials, 1503 participants) unless prehabilitation included exercise training, resulting in a small reduction in hospital LOS (SMD -0.91, 95% CI -1.67 to -0.14, I2 = 15.5%) (10 trials, 906 participants). Prehabilitation did not reduce ICU LOS (SMD -0.02, 95% CI -0.36 to 0.33, I2 = 31.68%)(5 trials, 1098 participants).
There are lower odds of developing PPC and all-cause complications when patients with sarcopenia or frailty undergo prehabilitation before upper abdominal surgery compared to no prehabilitation. There is a small reduction in hospital LOS (0.91 days) when prehabilitation includes exercise compared to no exercise intervention.
Amirkhosravi, F., Allenson, K.C., Moore, L.W. et al. Multimodal prehabilitation and postoperative outcomes in upper abdominal surgery: systematic review and meta-analysis. Sci Rep 14, 16012 (2024). https://doi.org/10.1038/s41598-024-66633-6

Preoperative respiratory muscle training reduces the risk of pulmonary complications and the length of hospital stay after cardiac surgery
This systematic review aimed to estimate the effect of preoperative respiratory muscle training (RMT) compared to no intervention on the incidence of post-operative pulmonary complications (PPC), post-operative length of stay, respiratory muscle strength and duration of mechanical ventilation in people following elective open cardiac surgery.
Guided by a prospectively registered protocol, database searches were conducted combining terms related to cardiac surgery, RMT and randomised controlled trials in 12 databases, including Cochrane Central Register of Trials, PubMed/Medline, Embase and PEDro from their inception until July 2021, two clinical trials registers and citation tracking. Two independent authors assessed potential eligible trials against predetermined criteria, methodological quality (using the PEDro scale) and extracted data. The participants were adults undergoing elective open heart surgery with or without cardiopulmonary bypass. RMT was defined as training delivered by inspiratory pressure loading (pressure threshold training), hyperpnoea with normocapnia or inspiration with resistance to flow. The comparison group received no intervention or sham RMT. Primary outcome measures were post-operative pulmonary complications (PPC), length of stay and respiratory muscle strength. Post-operative pulmonary complications were defined as pneumonia, hypoxaemia, hypercarbia, bronchospasm, atelectasis and respiratory failure. Meta-analyses were performed using a random-effects model to obtain effect sizes and their respective 95% confidence intervals (CI). Dichotomous outcomes were reported as risk ratios and continuous outcomes were reported using mean difference. Heterogeneity was assessed using the I-squared statistic. The overall quality of the evidence assessment was assessed using the GRADE approach.
Eight randomised controlled trials were included in the systematic review, published between 1998 and 2019. The eight trials contained data for 696 participants, with a mean age range of 59 to 71 years. Ninety percent of participants underwent coronary artery bypass grafts, 7% underwent valve replacements and the remaining 3% combined surgeries. Trials were from Brazil and the Netherlands (n=3), China (n=1) and the remaining from Israel (n=4). PEDro scores of the included trials ranged from four to eight in quality.
The dose of RMT varied across the eight trials. The initial training pressure commenced at 15% of maximal inspiratory pressure (MIP) (n=1), 30% (n=6) and 40% (n=1). The intervention duration ranged from 5 days (n=1), 2 weeks (n=3) and between 2 to 4 weeks (n=4). Training sessions ranged from one per day up to three times a day, and the training ranged from 3 x 10 inspirations to 30mins. Mortality was reported in 2 trials, with 5 deaths in the control group and 3 in the experimental group.
Compared to no intervention, there was moderate-quality evidence from six trials of 645 participants that RMT lowered the risk of PPC (RR 0.51, 95% CI 0.38 to 0.70) and high-quality evidence that RMT lowered the risk of pneumonia (RR0.44, 95% CI 0.25 to 0.78). There was high-quality evidence from four trials of 531 participants that RMT resulted in shorter hospital length of stay (MD -1.7 days, 95% CI -2.4 to -1.1).
The review concluded that RMT resulted in worthwhile improvements in outcomes that matter to patients. The risk of PPC in general and pneumonia were each reduced by about half, length of hospital stay was reduced by almost 2 days. These results were based on high-certainty evidence with low heterogeneity.
Cursino de Moura JF, Oliveira CB, Coelho Figueira Freire AP, Elkins MR, Pacagnelli FL (2024) Preoperative respiratory muscle training reduces the risk of pulmonary complications and the length of hospital stay after cardiac surgery: a systematic review. Journal of Physiotherapy 70:16–24
PEDro acknowledges this systematic review summary was prepared by Dr Tiffany Dwyer and Sandeep Gupta from the PEDro Education and Training Committee.

Exercise‐based cardiac rehabilitation for adults with heart failure
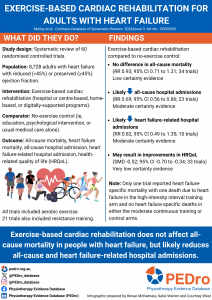
People with heart failure have low exercise tolerance, poor health-related quality of life (HRQoL), increased risk of mortality and hospital admission, and high healthcare costs. A Cochrane review in 2018 found that exercise-based cardiac rehabilitation (ExCR) compared to no exercise control improved HRQoL and hospital admissions, as well as a possible reduction in mortality. However, the RCTs included disproportionately represented populations, and were mostly conducted in a hospital or centre-based setting. This systematic review aimed to assess the effects of ExCR on mortality, hospital admissions, and health-related QoL in adults with heart failure.
This review included randomised controlled trials (RCTs) comparing ExCR with a follow-up of six months or longer versus a no-exercise control in people ≥18 years with heart failure (either heart failure with reduced (<45%) ejection fraction (HFrEF) or heart failure with preserved (≥45%) ejection fraction (HFpEF)). Six databases and two trial registers were searched for RCTs. There were no language or date restrictions. The exercise-based interventions were either given alone or as part of comprehensive cardiac rehabilitation in hospital or centre-based settings, as well as including alternative modes of delivery including home‐based and digitally‐supported programs. Usual care consisted of active interventions such as education or psychological intervention or usual medical care alone. The primary outcomes were all‐cause mortality, heart failure mortality, number of participants who experienced an all‐cause hospital admission, number of participants who experienced a heart failure‐related hospital admission, and HRQoL assessed by a validated outcome measure. Data was processed in accordance with the Cochrane Handbook for Systematic Reviews of Interventions, and The Cochrane Risk of Bias 1.0 tool was used to assess the level of bias. Data was pooled from trials using a random effects model, and a meta-analysis was performed. GRADE was used to assess the certainty of the evidence.
Sixty trials, involving 8,728 participants, were included with a median of six months follow-up. Aerobic exercise was included in all trials, with 21 trials also including resistance training. The exercise dosage across trials varied: time 8-120 minutes duration, frequency 1-7 sessions a week, intensity 40-80%, maximal heart rate to 50-85% maximal oxygen uptake (Vo2 max), and duration 8-120 weeks. The overall risk of bias was low or unclear, with the main issues found in trials to be poorly reported details surrounding random sequence generation, allocation concealment, and blinding.
There was no evidence of a difference in the short term (up to 12 months’ follow‐up) in the pooled risk of all‐cause mortality when comparing ExCR versus usual care (risk ratio (RR) 0.93; 95% confidence interval (CI) 0.71 to 1.21; p=0.95; I²=0%; 34 trials, 3941 participants; low certainty evidence). Only one trial reported heart failure‐specific mortality with one death due to heart failure in the high‐intensity interval training arm, and no heart failure‐specific deaths in either the moderate continuous training or control arms. Participation in ExCR versus usual care likely reduced the risk of all‐cause hospital admissions (RR 0.69; 95% CI 0.56 to 0.86; p=0.14, I²=24%; 23 trials; 2283 participants; moderate certainty evidence) and heart failure‐related hospital admissions (RR 0.82, 95% CI 0.49 to 1.35; p=0.41; I²=4%; 10 trials; 911 participants; moderate certainty evidence) in the short term. ExCR may improve HRQoL in the short term, but the evidence is very uncertain (standardised mean difference (SMD) −0.52; 95% CI −0.70 to −0.34; 33 trials; 4769 participants; very low certainty evidence).
Compared to no-exercise control, there was no evidence of a difference in all-cause mortality following ExCR in people with heart failure. ExCR likely reduced all-cause hospital admissions and heart failure-related hospital admissions and may result in improvements in HRQoL.
Molloy C, Long L, Mordi IR, Bridges C, Sagar VA, Davies EJ, Coats AJS, Dalal H, Rees K, Singh SJ, Taylor RS. Exercise‐based cardiac rehabilitation for adults with heart failure. Cochrane Database of Systematic Reviews 2024, Issue 3. Art. No.: CD003331. DOI: 10.1002/14651858.CD003331.pub6.
PEDro acknowledges Dr Renae McNamara, Clinical Specialist Physiotherapist, Prince of Wales Hospital and Katie Warren, Masters of Physiotherapy Student, University of Technology Sydney for preparing the summary.
Exercise-based rehabilitation programmes for pulmonary hypertension
This Cochrane systematic review aimed to estimate the effects of supervised exercise-based rehabilitation compared with usual care or no exercise-based rehabilitation on the primary outcomes; exercise capacity, serious adverse events and health-related quality of life in people with pulmonary hypertension.
This review included randomised controlled trials that assessed supervised exercise-based rehabilitation for people with pulmonary hypertension. Eligible trials were identified from five electronic databases. Trials were included if they compared supervised exercise-based rehabilitation of any duration, frequency or setting to a control group of education or usual care with no specific exercise component. Primary outcomes were; exercise capacity, which included measures such as the six-minute walk test and peak exercise capacity; serious adverse events during the intervention period, defined as mortality, disease progression, symptoms precluding training, and discontinuation of the study; and health-related quality of life, which was measured with any validated generic or disease specific quality of life measure.
Two reviewers independently identified and selected studies, extracted data, and assessed risk of bias using the Cochrane Risk of Bias 1.0 tool. Certainty of the evidence was evaluated using the GRADE framework.
The review included 14 trials (574 participants), of which 11 trials (462 participants) contributed to the meta-analyses. The mean age of participants ranged from 35 to 68 years and all trials included participants who were classified as being stable on medical therapy. Exercise-based programmes included both inpatient- and outpatient-based rehabilitation that incorporated both upper and lower limb exercise.
For the outcome exercise capacity, there is low certainty that supervised exercise-based rehabilitation compared with control may increase mean six-minute walk distance (MD 48.52 metres, 95% CI 33.42 to 63.62; 11 studies, 418 participants), may increase mean peak oxygen uptake (MD 2.07 mL/kg/min, 95% CI 1.57 to 2.57; 7 studies, 314 participants) and may increase mean peak power (MD 9.69 W, 95% CI 5.52 to 13.85; 5 studies, 226 participants).
For the outcome serious adverse events, there was moderate certainty that supervised exercise-based rehabilitation compared with control was probably not associated with an increased risk of serious adverse events (RD 0, 95% CI −0.03 to 0.03; 11 studies, 439 participants).
For the outcome health-related quality of life, there was moderate certainty that supervised exercise-based rehabilitation compared with control probably increases the 36-item Short Form Physical Component Score (MD 3.98 points, 95% CI 1.89 to 6.07; 5 studies, 187 participants) and the 36-item Short Form Mental Component Score (MD 3.60 points, 95% CI 1.21 to 5.98 points; 5 RCTs, 186 participants).
In people with pulmonary hypertension who are medically stable, supervised exercise-based rehabilitation may result in a large increase in exercise capacity, it is probably safe and probably improves quality of life.
Morris NR, Kermeen FD, Jones AW, Lee JYT, Holland AE. Exercise-based rehabilitation programmes for pulmonary hypertension. Cochrane Database of Systematic Reviews 2023, Issue 3. Art. No.: CD011285. DOI: 10.1002/14651858.CD011285.pub3.

Physical activity and exercise training in cystic fibrosis
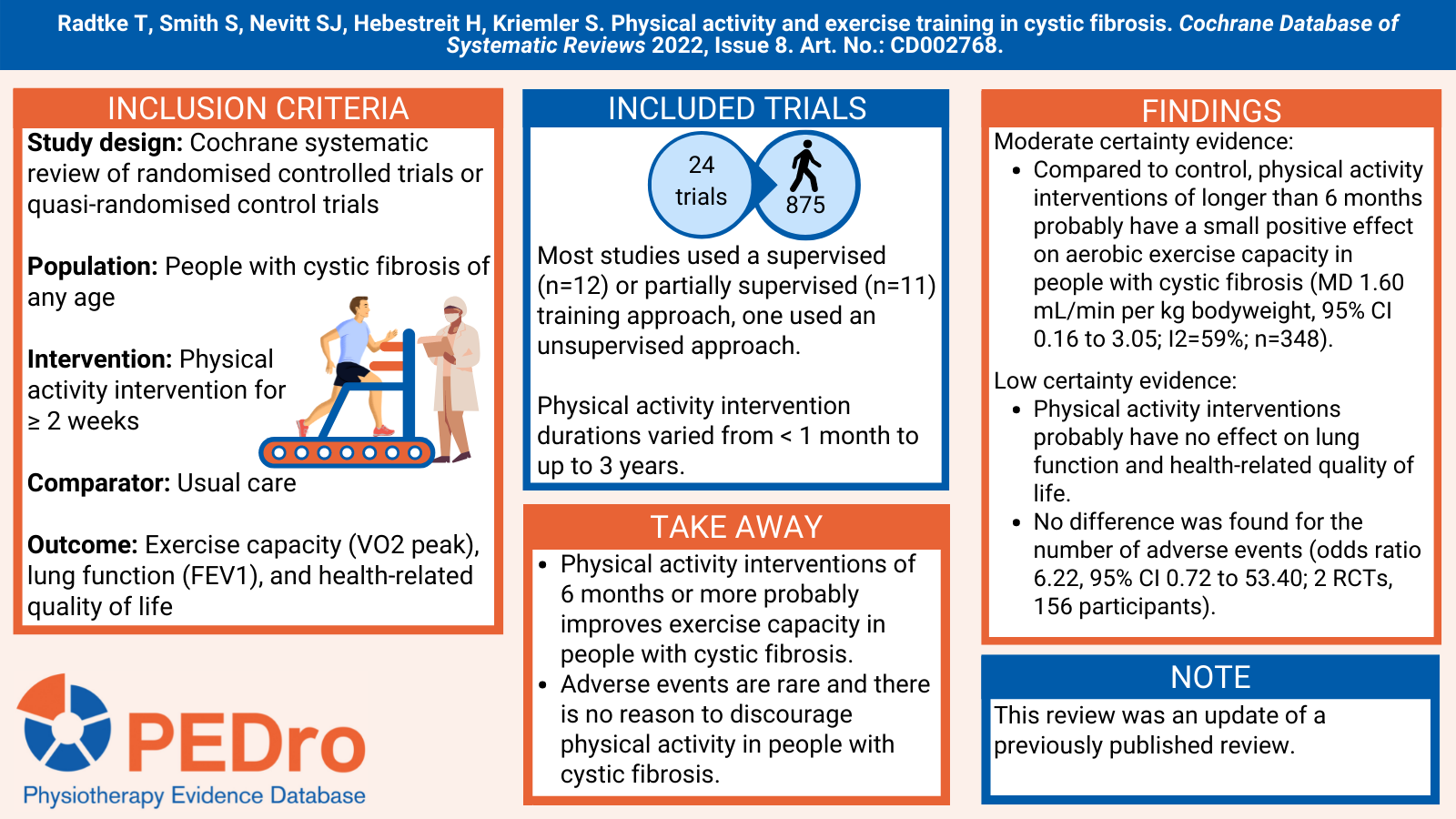
This Cochrane systematic review aimed to estimate the effects of physical activity on exercise capacity, lung function and health-related quality of life in people with cystic fibrosis. This review was an update of a previously published review.
This was a Cochrane systematic review of randomised controlled trials (RCTs) or quasi-randomised controlled trials. Relevant trials were identified from three trial registries. Trials were included if they included people with cystic fibrosis (of any age) who underwent any type of physical activity intervention compared to usual care (no physical activity intervention). Interventions needed to be two weeks or more in duration. The primary outcomes were exercise capacity (VO2 peak), lung function (FEV1), and health-related quality of life (using generic or disease-specific instruments).
Two review authors independently assessed studies for inclusion, extracted data, and undertook the assessment of risk of bias of included studies. Risk of bias was evaluated using the Cochrane risk of bias tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
There were 24 parallel RCTs included in the review (875 participants). Trial size varied from 9 participants to 117 participants and included a mix of adults, children, and adolescents. 12 studies used a supervised training approach, 11 used a partially supervised approach and one study used an unsupervised approach. Physical intervention durations varied from less than a month to up to 3 years.
Compared to no physical activity intervention (usual care), there was moderate certainty evidence that physical activity interventions of longer than 6 months probably have a small positive effect on aerobic exercise capacity in people with cystic fibrosis (MD 1.60 mL/min per kg bodyweight, 95% CI 0.16 to 3.05; I2=59%; n=348). There was low certainty evidence that physical activity interventions probably have no effect on lung function and health-related quality of life. No difference between groups was found for the number of adverse events over six months (odds ratio 6.22, 95% CI 0.72 to 53.40; 2 RCTs, 156 participants; low-certainty evidence).
Physical activity interventions of 6 months or more probably improves exercise capacity in people with cystic fibrosis. Adverse events are rare and there is no reason to discourage physical activity in people with cystic fibrosis.
Radtke T, Smith S, Nevitt SJ, Hebestreit H, Kriemler S. Physical activity and exercise training in cystic fibrosis. Cochrane Database of Systematic Reviews 2022, Issue 8. Art. No.: CD002768. DOI: 10.1002/14651858.CD002768.pub5.
Rehabilitation to enable recovery from COVID-19
COVID-19 was declared a pandemic by the World Health Organization on 11 March 2020. Physiotherapy consensus guidelines were quickly developed to guide acute respiratory management for those with COVID-19. When managing a new disease like COVID-19, health professionals can utilise high-quality clinical research evaluating the management of similar patient groups (eg, those admitted to an intensive care unit with severe respiratory illness). This systematic review aimed to estimate the effects of rehabilitation interventions compared to usual care on functional ability and quality of life in people with severe respiratory illness and consider whether this evidence was generalisable to people with severe COVID-19. A secondary aim was to explore the views and experiences of those undergoing rehabilitation.
Guided by a prospectively registered protocol, Cochrane guidance for rapid reviews and the PRISMA guidelines, sensitive searches were performed in 7 databases (including Medline and PEDro) to 7 May 2020. Systematic reviews and randomised controlled trials that evaluated any rehabilitation intervention aimed at enhancing or restoring physical impairment or disability in adults with severe respiratory illness requiring intensive or critical care (eg, severe adult respiratory distress syndrome) were included. Interventions were classified as: fitness, balance or strengthening exercise; mobility training; early mobilisation; neuromuscular electrical stimulation; insufficient information to categorise. Interventions that used a combination of these were classified as multicomponent. The intervention could be applied in any setting, including in the intensive care unit, in a sub-acute hospital ward, as an outpatient, at home, or any combination of these settings. Qualitative studies were also included if they explored the patient experience of rehabilitation. The comparator was usual care. The primary outcomes were functional ability and quality of life. Two independent reviewers screened 25% of the search results. The remaining 75% were screened by a single reviewer and a second reviewer checked the excluded articles. Data were extracted by a single reviewer and checked by a second reviewer. A third reviewer was involved where necessary. Quality was assessed using the Critical Appraisal Skills tools. A narrative synthesis was undertaken, organised by age and intervention type and setting.
23 systematic reviews (61 unique randomised controlled trials), 11 additional trials (993 participants) and 8 qualitative studies (99 participants) were included in the narrative synthesis. The quality of the reviews was generally good, but the additional trials and qualitative studies were more variable. The most common intervention was early mobilisation (9 reviews, 3 qualitative) followed by multicomponent intervention (6 reviews, 2 trials), exercise and early mobilisation (3 reviews, 2 trials), neuromuscular electrical stimulation (3 reviews, 2 trials), and fitness, balance or strengthening exercise (4 trials, 1 qualitative). There was insufficient information provided to categorise the intervention for 2 reviews, 1 trial and 4 qualitative studies. The interventions were mostly implemented in the intensive care unit (17 reviews, 6 trials, 4 qualitative).
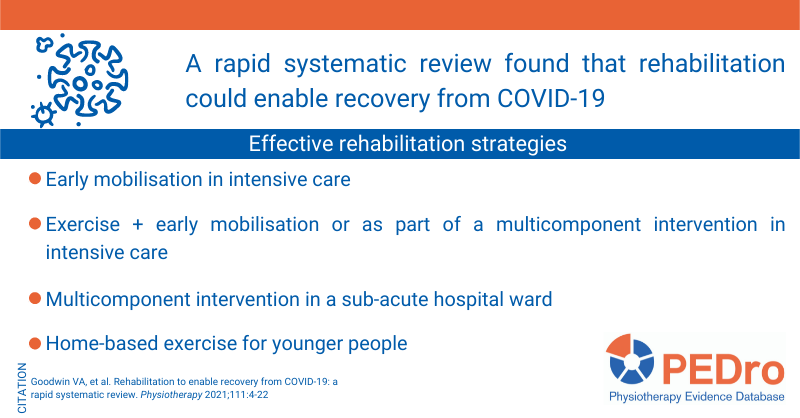
Early mobilisation in intensive care may decrease intensive care acquired weakness and improve functional ability. Within 72 to 96 hours of starting mechanical ventilation appears to be the optimal time to commence this intervention. More information about the effects of early mobilisation is available in a PEDro blog. Exercise combined with early mobilisation or as part of a multicomponent intervention in intensive care can improve strength and independent walking, while multicomponent intervention may improve activities of daily living when applied in a sub-acute hospital ward and improve respiratory function when home-based. Progressive fitness, balance and strength exercise delivered in intensive care can improve functional independence. Home-based exercise may increase functional capacity in younger patients, but the findings are inconclusive for older patients. The findings are inconclusive for neuromuscular electrical stimulation in the intensive care setting, but may improve strength in older patients in the sub-acute hospital ward setting. Findings regarding quality of life were inconclusive.
The qualitative studies revealed that people receiving rehabilitation valued it. A consistent theme was that individually tailored interventions encouraged hope and confidence.
Exercise, early mobilisation and multicomponent rehabilitation programs may improve recovery following admission to intensive care for severe respiratory illness. This evidence can be generalised to people with, or recovering from, COVID-19.
Goodwin VA, et al. Rehabilitation to enable recovery from COVID-19: a rapid systematic review. Physiotherapy 2021;111:4-22
Watch or listen to an interview with Vicki Goodwin about the review:
Efficacy of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery
Prehabilitation aims to promote physical and psychological health and address modifiable risk factors prior to surgery to improve postoperative outcomes. There are conflicting results regarding the effectiveness of prehabilitation in patients with cancer awaiting surgery, and the optimal approach to delivering prehabilitation is unclear. This systematic review aimed to estimate the effects of exercise prehabilitation compared to standard care on postoperative outcomes in adults undergoing surgery for abdominal cancer.
Guided by a prospectively registered protocol, citation tracking and sensitive searches were conducted in 5 databases (including Medline and PEDro) to identify (pseudo-)randomised controlled trials that investigated the effects of exercise prehabilitation for adults scheduled to undergo abdominal surgery for cancer. Exercise prehabilitation could involve any form of exercise (including whole body or respiratory exercise) plus education and be delivered either as a stand-alone intervention (ie, unimodal) or included within a framework of multimodal interventions (ie, with nutritional or psychological interventions). The comparator was not exposed to a prehabilitation program, like standard care or no intervention. The outcomes included functional capacity (eg, 6-Minute Walk Test), cardiorespiratory fitness (eg, VO2peak), postoperative complications, hospital length of stay, hospital re-admission, and postoperative mortality, but the primary outcome was not identified. The Consensus Exercise Reporting Template was used to extract information about the interventions. Risk of bias of the included trials was evaluated using version 2 of the Cochrane risk of bias tool. Two reviewers independently selected trials for inclusion, extracted data and evaluated risk of bias. Disagreements were resolved by consensus or by arbitration from a third reviewer. Meta-analyses were performed for each outcome, calculating the mean differences (when data were reported for the same scale), standardised mean differences (when data were reported using different scales) or odds ratios (for dichotomous variables) and their associated 95% confidence intervals (CI). Certainty of evidence was evaluated using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. Three subgroup comparisons were pre-planned: low vs. high functional capacity at baseline; shorter vs. longer prehabilitation programs; and, unimodal vs. multimodal programs.
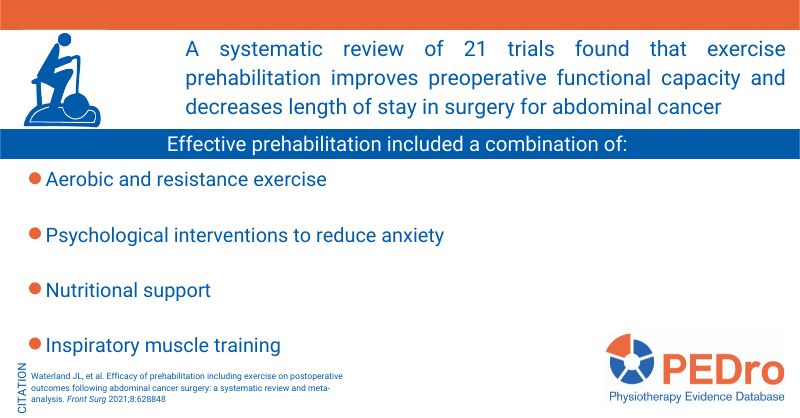
21 trials (1,640 participants) were included in the meta-analysis. Most trials were from Canada (5) or the United Kingdom (5). The type of cancer was colorectal (7 trials), gastro-oesophageal (4), urological (4), other specific cancer (3) or a variety of cancers (3). 9 trials evaluated unimodal exercise prehabilitation and 12 were multimodal. Exercise involved aerobic and strength training (9 trials), aerobic training (5), aerobic, strength and respiratory training (4), respiratory training (2) or education (1). Intervention was commonly provided in a home-based setting by physiotherapists. The frequency and duration of programs generally ranged from five sessions over 1 week to three times/week for 8 weeks.
Compared to standard care, prehabilitation increased preoperative functional capacity by 34 metres on the 6-Minute Walk Test (95% CI 19 to 49; 522 participants; 8 trials; moderate certainty) and reduced postoperative hospital length of stay by a mean of 3.7 days (0.9 to 6.4; 458 participants; 4 trials; moderate certainty). In contrast, there was no difference between standard care and prehabilitation for preoperative cardiorespiratory fitness (mean difference for VO2peak 1.7 ml/min/kg; -0.0 to 3.5; 121 participants; 3 trials; low certainty), postoperative complications (odds ratio 0.81, 95% CI 0.55 to 1.18; 917 participants; 16 trials; low certainty), hospital re-admission (odds ratio 1.07, 0.61 to 1.90; 464 participants; 6 trials; moderate certainty), and postoperative mortality (odds ratio 0.95; 95% CI 0.43 to 2.09; 901 participants; 7 trials; low certainty).
Subgroup comparison was possible for unimodal vs. multimodal programs for functional capacity (6-Minute Walk Test). Compared to standard care, multimodal programs increased the distance walked in 6 minutes by a mean of 33 metres (95% CI 18 to 49; 464 participants; 6 trials) compared to 52 metres (-13 to 116; 58 participants; 2 trials) for unimodal programs. However, this finding should be interpreted with caution because of the small number of participants and trials available for unimodal programs.
Exercise prehabilitation, particularly multimodal approaches, improves preoperative functional capacity and reduces postoperative hospital length of stay in people undergoing surgery for abdominal cancer.
Waterland JL, et al. Efficacy of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery: a systematic review and meta-analysis. Front Surg 2021;8:628848
Effectiveness of aerobic exercise on smoking cessation in adults
Smokers tend to have unhealthy habits, including being physically inactive. The combination of smoking and physical inactivity increases the risk of developing chronic diseases. Aerobic exercise may assist smokers to quit. This systematic review aimed to estimate the effects of aerobic exercise compared to usual care on smoking cessation in adults.
Guided by a prospectively registered protocol, citation tracking plus sensitive searches of 6 databases and 4 trial registries were performed to identify randomised controlled trials evaluating aerobic exercise for smoking cessation. To be included, the trials needed to compare aerobic exercise (with or without nicotine therapy replacement) to usual care (with or without nicotine replacement). The aerobic exercise could be delivered with co-interventions, including behavioural support and drug therapy. Usual care was defined as any behavioural support, including educational classes, lectures and health orientations, social support, and strategies for replacing cigarettes. The primary outcome was smoking cessation defined as the prevalence of those reporting abstinence in the short (< 3 months), medium (3-12 months) and long (> 12 months) term. Two reviewers independently selected trials for inclusion, extracted data, and evaluated trial quality and certainty of evidence. Disagreements were resolved by a third reviewer. Trial quality was evaluated using the PEDro scale. Certainty of the evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Meta-analysis was performed to calculate the risk ratio and 95% confidence interval (CI) in the short, medium and long term.
11 trials involving 2,093 participants were included in the meta-analysis. Average participant age ranged from 37 to 48 years. 6 trials exclusively recruited women and 5 recruited a combination of men and women. Aerobic exercise was performed in group sessions in all trials. Average session duration was 20-60 minutes, with 1-6 sessions/week for 7-15 weeks.
Aerobic exercise was better than usual care in achieving smoking cessation at short term, with a risk ratio of 0.79 (95% CI 0.66 to 0.94; 11 trials; 1,945 participants; moderate certainty). In contrast, there were no differences between aerobic exercise and usual care in the medium (risk ratio 0.91; 95% CI 0.72 to 1.15; 9 trials; 1,486 participants; moderate certainty) and long (risk ratio 0.96; 95% CI 0.78 to 1.18; 7 trials; 1,529 participants; moderate certainty) term.
Aerobic exercise (combined with behavioural support and drug therapy) can be used to aid smoking cessation during the first 3 months of cessation.
Santos CP, et al. Effectiveness of aerobic exercise on smoking cessation in adults: a systematic review and meta-analysis. J Phys Act Health 2021;18(2):230-42
Advanced telehealth technology improves home-based exercise therapy for people with stable chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease is a major cause of disability and mortality worldwide. There is level 1 evidence that exercise-based pulmonary rehabilitation improves exercise capacity, dyspnoea and quality of life. Telecommunication technology can be used to deliver exercise therapy. This systematic review aimed to estimate the effects of exercise therapy delivered using advanced telehealth technology compared to no exercise or inpatient or outpatient exercise therapy and home-based exercise therapy without telehealth on exercise capacity, quality of life, dyspnoea and costs in people with stable chronic obstructive pulmonary disease.
Guided by a prospectively registered protocol, sensitive searches were performed in 7 databases (including Medline and PEDro), hand searching of relevant conference proceedings and citation tracking. Randomised controlled trials involving people with stable chronic obstructive pulmonary disease were included if they compared exercise therapy delivered using advanced telehealth technology to: (1) no exercise, (2) inpatient or outpatient exercise therapy, or (3) home-based exercise therapy without telehealth. Exercise therapy delivered using advanced telehealth technology was defined as delivery of home-based exercise using any telehealth technology that was more advanced than phone contact alone (eg, real-time videoconferencing, web-based interactive platforms or smartphone applications providing either therapist or algorithm-mediated (automated) individualised feedback and goals). The primary outcomes were exercise capacity, quality of life, dyspnoea and costs in the short (1-4 months) and long (9-12 months) term. Two reviewers independently selected trials, extracted data, and evaluated trial quality and certainty of evidence, with any disagreements resolved by discussion or arbitration by a third reviewer. Trial quality was evaluated using the Cochrane risk of bias tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Meta-analysis was used to estimate the mean difference and 95% confidence interval (CI) for each outcome for each comparison.
34 articles reporting 15 trials (1,522 participants) were included in the analyses. Exercise therapy delivered using advanced telehealth technology was compared to no exercise in 7 trials, to inpatient or outpatient exercise therapy in 3 trials, and to home-based exercise therapy without telehealth in 6 trials (note, 1 trial compared exercise delivered with telehealth to both no exercise and home-based exercise without telehealth). The advanced telehealth technology consisted of real-time supervised/monitored exercise sessions (2 trials) and unsupervised training with telehealth feedback (13 trials). The dose of exercise training ranged from 3-7 sessions/week for 1-12 months.
Exercise therapy delivered using advanced telehealth technology increased the distance walked in 6 minutes (mean difference 15 m; 95% CI 5 to 24; 4 trials; 458 participants; low certainty) and improved quality of life measured using the St George Respiratory Questionnaire (mean difference -4%; 95% CI -7 to 0; 4 trials; 361 participants; low certainty) and dyspnoea measured using the Chronic Respiratory Questionnaire dyspnoea sub-score (mean difference 2 points; 95% CI 0 to 4; 2 trials; 120 participants; very low certainty) in the short term compared to no exercise therapy. Meta-analyses could not be performed for the long-term outcomes and there were no data available for cost-effectiveness.
Compared to inpatient or outpatient exercise therapy, exercise therapy delivered using advanced telehealth technology produced a similar distance walked in 6 minutes (mean difference 6 m; 95% CI -26 to 37; 2 trials; 224 participants; low certainty) and modified Medical Research Council dyspnoea scale score (mean difference 0 points; 95% CI 0 to 0; 2 trials; 152 participants; low certainty) but improved quality of life measured with the St George Respiratory Questionnaire score (mean difference -4%; 95% CI -9 to 0; 2 trials; 224 participants; low certainty) in the short-term. Again, meta-analyses could not be performed for the long-term outcomes and there were no data available for cost-effectiveness.
Exercise therapy delivered using advanced telehealth technology had a similar effect as home-based exercise therapy without technology on distance walked in 6 minutes (mean difference 2 m; 95% CI -16 to 19; 3 trials; 231 participants; low certainty) and St George Respiratory Questionnaire score (mean difference -14%; 95% CI -28 to 1; 3 trials; 171 participants; very low certainty) but improved the Chronic Respiratory Questionnaire dyspnoea sub-score (mean difference 2 points; 95% CI 0 to 4; 2 trials; 123 participants; very low certainty) in the short term. One trial (105 participants) reported cost-effectiveness, with no difference in total cost (mean difference EUR -288; 95% CI -3,998 to 3,424). Meta-analyses could not be performed for the long-term outcomes.
Exercise therapy delivered using advanced telehealth technology may improve exercise capacity, dyspnoea and quality of life compared with no exercise therapy, although some benefits may be small. Exercise therapy delivered using advanced telehealth technology is generally similar to inpatient or outpatient exercise therapy, and similar to or better than home-based exercise therapy without technology.
Bonnevie T, et al. Advanced telehealth technology improves home-based exercise therapy for people with stable chronic obstructive pulmonary disease: a systematic review. J Physiother 2021;67(1):27-40
Pulmonary rehabilitation can improve the functional capacity and quality of life for pneumoconiosis patients
Pneumoconiosis is a class of interstitial lung disease where inhalation of mineral dust (eg, silica) has caused interstitial fibrosis. It is commonly caused by occupational exposure. In 2018 pneumoconiosis accounted for over 80% of occupational diseases recorded in China. This systematic review aimed to estimate the effects of pulmonary rehabilitation compared to routine treatment on functional capacity and quality of life in people with pneumoconiosis.
Guided by a prospectively registered protocol, sensitive searches were performed in nine databases (including PubMed, Embase and Cochrane CENTRAL), three trial registries, and citation tracking of included trials and existing systematic reviews. To be included, trials needed to have compared pulmonary rehabilitation to routine treatment in people with pneumoconiosis. Pulmonary rehabilitation had to include exercise training, and could also include health education, nutritional intervention and psychosocial support. The primary outcomes were functional capacity (measured by the 6-minute walk test) and quality of life (measured by the St George’s Respiratory Questionnaire). Two reviewers independently selected trials, extracted data and evaluated trial quality. Disagreements were resolved by discussion or by a third reviewer. Trial quality was assessed using the Cochrane risk of bias tool. Certainty of the evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. Meta-analysis was used to calculate the mean between-group difference and 95% confidence interval (CI). Two subgroup analyses were performed to evaluate the: (1) content of the intervention (exercise training combined with health education vs. exercise training combined with health education plus other interventions); and (2) duration of intervention (< 3 months vs. >= 3 months).
16 trials (1,307 participants) were included in the analyses. All but one trial were conducted in China. The duration of pulmonary rehabilitation ranged from 1.5 to 12 months, with 6 trials using a duration of < 3 months and 10 trials a duration of >= 3 months. The most common content of the pulmonary rehabilitation interventions evaluated were exercise training combined with health education and respiratory training (6 trials) and exercise training in combination with health education (5 trials).
Compared to routine treatment, pulmonary rehabilitation increased the distance walked in a 6-minute walk test by a mean of 69 m (95% CI 62 to 76; 12 trials; 1,049 participants; moderate certainty) and improved the St George’s Respiratory Questionnaire score by a mean of -10 points (-16 to -3; 4 trials; 540 participants; very low certainty). The subgroup analyses produced similar results for both the content and duration of the intervention. For the 6-minute walk test, exercise training combined with health education increased the distance by 64 m (53 to 75; 6 trials; 525 participants) while exercise training combined with health education plus other interventions increased by 74 m (64 to 83; 6 trials; 524 participants). Pulmonary rehabilitation of < 3 months duration increased walking distance by 71 m (58 to 85; 5 trials; 533 participants) compared to 67 m (58 to 77; 7 trials; 516 participants) for >= 3 months duration. For the St George’s Respiratory Questionnaire, exercise training combined with health education improved the total score by -10 points (-23 to 3; 2 trials; 300 participants) while exercise training combined with health education plus other interventions improved it by -9 points (-22 to 3; 2 trials; 240 participants). Pulmonary rehabilitation of < 3 months duration improved the St George’s Respiratory Questionnaire score by -4 points (-6 to -1; 2 trials; 360 participants) whereas the effect was -17 points (-21 to -12; 2 trials; 180 participants) for programs with >= 3 months duration. Adverse events were not documented by any of the included trials.
Pulmonary rehabilitation probably improves functional capacity and may improve quality of life in patients with pneumoconiosis.
Zhao H, et al. Pulmonary rehabilitation can improve the functional capacity and quality of life for pneumoconiosis patients: a systematic review and meta-analysis. BioMed Res Int 2020;(6174936):Epub
Early rehabilitation reduces the likelihood of developing intensive care unit-acquired weakness
Intensive care unit-acquired weakness is associated with significant impairments in body structure and function, activity limitation, and participation restriction. The aim of this review was to estimate the average effect of early rehabilitation interventions compared to usual care on the incidence of intensive care unit-acquired weakness in critically ill patients.
Sensitive searches were performed in five databases (including Medline, Cochrane CENTRAL, and PEDro). Randomised controlled trials of early rehabilitation intervention (early mobilisation and/or neuromuscular electrical stimulation) in critically ill adults who had not already been diagnosed with intensive care unit-acquired weakness that measured muscle strength were included. The primary outcome was the incidence of intensive care unit-acquired weakness. Secondary outcomes included length of time on mechanical ventilation, discharge location, length of stay (both in intensive care and in hospital), and acute mortality (death in intensive care or hospital). Two reviewers independently identified trials for inclusion, extracted data, and assessed trial quality. Discrepancies were resolved through discussion or by arbitration from a third reviewer. The Cochrane risk of bias tool was used to evaluate trial quality. Meta-analysis was used to calculate the odds ratio and 95% confidence interval (CI) for the incidence of intensive care unit-acquired weakness. Four subgroup analyses were performed: (1) < = 7 vs. > 7 day length of stay in intensive care; (2) intervention starting < = 72 hours vs. > 72 hours of admission to intensive care; (3) the type of intervention (early mobilisation vs. neuromuscular electrical stimulation vs. early mobilisation and neuromuscular electrical stimulation); and, (4) time point for assessing intensive care unit-acquired weakness (awakening, 7th day post-awakening, intensive care discharge, hospital discharge).
Nine trials (841 participants) were included in the analyses. Most participants had received mechanical ventilation. The intervention was progressive early mobilisation exercise in five trials, neuromuscular electrical stimulation in three trials, and a combination of early mobilisation and neuromuscular electrical stimulation in one trial. The control group received early mobilisation interventions as part of usual care in six trials.
Early rehabilitation decreased the likelihood of developing intensive care unit-acquired weakness, with an odds ratio of 0.71 (95% CI 0.53 to 0.95, 9 trials). The effect size was larger for > 7 day length of stay in intensive care (odds ratio 0.51, 95% CI 0.32 to 0.81, 7 trials) compared to shorter stays (odds ratio 0.96, 95% CI 0.50 to 1.85, 2 trials), and when intervention commenced in < =72 hours of admission (odds ratio 0.57, 95% CI 0.37 to 0.88, 7 trials) compared to > 72 hours (odds ratio 0.70, 95% CI 0.17 to 2.84, 2 trials). The type of intervention had an impact on the effect size, with an odds ratio of 0.71 (95% CI 0.45 to 1.12, 5 trials) for progressive early mobilisation exercises, 0.26 (95% CI 0.09 to 0.80, 3 trials) for neuromuscular electrical stimulation, and 0.58 (95% CI 0.17 to 1.98, 1 trial) for a combination of early mobilisation and neuromuscular electrical stimulation. The effect size was largest at hospital discharge (odds ratio 0.37, 95% CI 0.15 to 0.94, 3 trials) compared to awakening (odds ratio 0.92, 95% CI 0.05 to 15.68, 2 trials), 7th day post-awakening (odds ratio 1.08, 95% CI 0.46 to 2.55, 1 trial), and intensive care discharge (odds ratio 0.78, 95% CI 0.49 to 1.24, 6 trials).
Early rehabilitation decreased the likelihood of developing intensive care unit-acquired weakness.
Anekwe DE, et al. Early rehabilitation reduces the likelihood of developing intensive care unit-acquired weakness: a systematic review and meta-analysis. Physiotherapy 2020;107:1-10
How does exercise treatment compare with antihypertensive medications?
This systematic review evaluated how different types and intensities of exercise compared against different classes and doses of antihypertensive medications in lowering systolic blood pressure levels. The review included randomised controlled trials that were conducted in adults with or without hypertension but no cardiovascular disease, cerebrovascular disease, diabetes or other chronic condition such as cancer. Any form of structured exercise and antihypertensive medication was considered to be included as the experimental intervention. Interventions were compared against usual practice (no exercise), other exercise regimens, or medications. Risk of bias was evaluated with the Cochrane risk of bias tool. A network meta-analysis was performed to compare the multiple interventions simultaneously.
The review included 197 trials of exercise (n = 10,461 participants) and 194 trials testing antihypertensive drugs (n = 29,281), totalling 391 trials included in the analysis (n = 39,742). No trials directly compared exercise and antihypertensive drugs. The average systolic blood pressure at baseline was 132 mmHg for participants in trials of exercise interventions, whereas in trials of antihypertensive medications it was consistently over 150 mmHg. The majority of trials tested endurance interventions (n = 135), such as walking, running, cycling or aquatic exercise.
Across all populations, both exercise interventions (mean difference -5 mmHg, 95% confidence interval -6 to -4) and antihypertensive medications (-9 mmHg, -10 to -8) were effective in lowering systolic blood pressure compared with control. Populations receiving medications achieved greater reductions in systolic blood pressure compared with those participating in exercise interventions (-4 mmHg, -5 to -3). All types of exercise lowered blood pressure in a similar fashion, with exception of the combination of endurance and resistance training which was more effective than dynamic resistance exercise alone (-3 mmHg, -5 to -1). A dose-response effect was observed for medications, but there was substantial uncertainty for effects of different intensities of exercise.
This review showed that the effect of exercise on lowering systolic blood pressure appears to be similar to that of commonly used antihypertensive medications across diverse populations and settings. The possibility of confounding due by the observed differences in trial populations and characteristics cannot be ruled out.
Network meta-analysis is explained in a PEDro blog from 2018.
Naci H, et al. How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br J Sports Med 2019;53(14):859-69
Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema
This Cochrane systematic review evaluated the effectiveness and safety of non-invasive positive pressure ventilation compared to standard care for adults with acute cardiogenic pulmonary oedema. Randomised controlled trials recruiting participants aged 18 years and older with a diagnosis of acute cardiogenic pulmonary oedema that evaluated nasal or face mask non-invasive positive pressure ventilation (continuous positive airway pressure, bilevel non-invasive positive pressure ventilation, or both) were included. Cross-over and cluster trials were excluded. The primary outcome was hospital mortality. Secondary outcomes included endotracheal intubation, incidence of acute myocardial infarction during hospitalisation, after starting treatment. The quality of the evidence was assessed using the GRADE approach.
24 trials (n = 2,664 participants) were included. Most trials were conducted in emergency departments or intensive care units. The mean age of the population was 73 (SD 9) years. There was low-quality evidence that non-invasive positive pressure ventilation may reduce hospital mortality compared to standard care (relative risk 0.65, 95% confidence interval (CI) 0.51 to 0.82; n = 2,484 participants; number needed to treat = 17). There was moderate quality evidence that non-invasive positive pressure ventilation probably reduces endotracheal intubation rates (RR 0.49 95% CI 0.38 to 0.62; n = 2,449 participants; number needed to treat = 13). There was moderate quality evidence that non-invasive positive pressure ventilation probably does not reduce the incidence of acute myocardial infarction compared to standard care (RR 1.03 95% CI 0.91 to 1.16; n = 1,313 participants; number needed to treat = 5). The use of non-invasive positive pressure ventilation in patients with acute cardiogenic pulmonary oedema may reduce mortality and probably reduces the risk of endotracheal intubation.
Berbenetz N et al. Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database Syst Rev 2019;Issue 4
Exercise therapy for functional capacity in chronic diseases
This umbrella review included 85 meta-analyses of randomised controlled trials evaluating the effectiveness of exercise therapy on functional capacity in people with chronic disease. Exercise therapy was compared with no treatment or usual care in adults with non-communicable chronic diseases defined by the World Health Organisation (WHO). The methodological quality of the included meta-analysis was evaluated using the AMSTAR checklist. The type of exercise therapy was classified into four categories: aerobic exercise, resistance training, aerobic and resistance training combined, and other condition-specific exercise-based training. The authors conclude that exercise therapy was effective for improving physical performance and functional capacity in all included chronic diseases (Alzheimer’s disease, cancer, chronic fatigue syndrome, chronic heart failure, chronic kidney disease, chronic obstructive pulmonary disease, cognitive impairment, coronary heart disease, dementia, fibromyalgia, interstitial lung disease, multiple sclerosis, osteoarthritis, Parkinson’s disease, peripheral arterial disease, rheumatoid arthritis, stroke, and type 2 diabetes). Around half of the effect estimates were of moderate to large magnitude and likely to be clinically important. Results were mostly similar among the different types of exercises, except for condition-specific programs that had a lower proportion of significant results compared with the others. Exercise also appears to be safe, but adverse events were not consistently reported. Exercise therapy should be recommended for people with chronic disease to improve functional capacity and reduce disability.
Pasanen T et al. Exercise therapy for functional capacity in chronic diseases: an overview of meta-analyses of randomised controlled trials. Br J Sports Med 2017;51:1459-65
Efficacy of different types of exercise-based cardiac rehabilitation on coronary heart disease
The aim of this network meta-analysis was to evaluate the effectiveness of centre-based, home-based and telephone-based cardiac rehabilitation in people with coronary heart disease. This review included randomized controlled trials of adult patients (18 years and older) with coronary heart disease that compared exercise-based cardiac rehabilitation with other cardiac rehabilitation modalities or usual care. Exercise-based cardiac rehabilitation modalities were classified as centre-based (cardiac rehabilitation undertaken in a hospital or centre with equivalent structure), home-based (cardiac rehabilitation undertaken at patients’ home or facilities other than hospitals, such as community centres) or telephone-based rehabilitation (cardiac rehabilitation undertaken at patients’ home but monitored and guided by health professionals using telehealth technologies. Risk of bias was assessed using the Cochrane risk of bias tool. Primary outcome was all-cause mortality. Pairwise meta-analysis were performed first to estimate the direct effect of the exercise-based interventions. Subsequently, a network meta-analysis was performed. In total, 60 randomised controlled trials were included (n = 19,411). Only half of the studies reported details of the exercise programs (types of exercise, frequency, lengths of sessions and duration of rehabilitation). Findings from the network meta-analysis showed that only centre-based cardiac rehabilitation significantly reduced all-cause mortality compared to usual care (relative risk 0.76, 95% CI 0.64 to 0.90), while the other types of cardiac rehabilitation were not significantly different from usual care with regard to mortality: home-based versus usual care (relative risk 0.86, 95% CI 0.55 to 1.33); telephone-based versus usual care (relative risk 0.97, 95% CI 0.62 to 1.52). This network meta-analysis showed that centre-based cardiac rehabilitation is the most appropriate therapeutic approach for patients with coronary heart disease.
Xia T-L, et al. Efficacy of different types of exercise-based cardiac rehabilitation on coronary heart disease: a network meta-analysis. J Gen Intern Med 2018;33(12):2201-9
Cardiac rehabilitation and physical activity
This review aimed to determine the impact of cardiac rehabilitation on physical activity levels of people with coronary heart disease and heart failure. The review included 47 randomised controlled trials (n = 6480 participants; 5825 coronary heart disease, 655 heart failure) that compared cardiac rehabilitation to control interventions. Meta-analysis was undertaken where two or more studies reported the same units of physical activity measurement (45 different measures were used). Outcomes were grouped into short-term (< 12 months) and long-term (> 12 months). 25 studies did not adequately report the description of randomisation, 27 studies had issues with concealment of allocation, and 26 studies did not report blinding of outcome assessment. Participation in cardiac rehabilitation increased the number of steps/day (mean difference 1423 steps, 95% CI 757 to 2089, 5 studies) and energy expenditure (mean difference 878 kcal/week, 95% CI 433 to 1323, 3 studies) in the short-term, plus increased the proportion of patients categorised as being physically active in the short-term (relative risk 1.55, 95% CI 1.19 to 2.02, 9 studies) and long-term (relative risk 1.48, 95% CI 1.19 to 1.83, 5 studies). Pooling from two studies indicated no effect of cardiac rehabilitation on sedentary time (mean difference -10.9 min/day, 95% CI -39 to 17), time spent in light intensity physical activity (mean difference -6.6 min/week, 95% CI -45 to 31), and time spent in moderate intensity physical activity (mean difference 8.5 min/week, 95% CI -1.44 to 18.44). In summary, this systematic review provided moderate evidence that cardiac rehabilitation increases physical activity levels compared with control interventions in people with coronary heart disease and heart failure.
Dibben GO et al. Cardiac rehabilitation and physical activity: systematic review and meta-analysis. Heart 2018;104(17):1394-402
Supervised exercise therapy versus home-based exercise therapy versus walking advice for intermittent claudication
This recent systematic review evaluates the effects of supervised exercise therapy compared to home-based exercise therapy and walking advice in people with intermittent claudication. This is an update of a Cochrane systematic review, which was first published in 2006. The primary outcome was maximal treadmill walking distance or time. Secondary outcomes were pain-free treadmill walking distance or time, quality of life, functional impairment, mortality and adherence to exercise program. Supervised exercise therapy was defined as a treatment program lasting at least 6 weeks with more than 50% of total exercise spent on walking or training the lower limbs and conducted under supervision of a physiotherapist or trained medical professional either as a hospital-based or community-based program. Home-based exercise therapy was defined as structured walking advice supplemented with an observation component (e.g., exercise log-book). Walking advice was defined as “go home and walk” advice provided with or without a predefined exercise scheme. The review identified 21 randomised controlled trials (1,400 participants), among which 635 received supervised exercise therapy, 320 home-based exercise therapy and 445 received walking advice. 17 trials (81%) were considered to be low risk of bias. There is moderate quality evidence showing that structured exercise therapy is superior to home-based exercise therapy (standardised mean difference 0.37; 95% confidence interval 0.12 to 0.62) and high quality evidence showing that supervised exercise therapy is superior to walking advice (standardised mean difference 0.80; 95% confidence interval 0.53 to 1.07) in improving maximal treadmill walking distance at three months. These effect sizes represent that participants treated with structured exercise therapy were able to walk 120 metres further than those treated with home-based exercise therapy and 210 meters more than those treated walking advice, on average. There is moderate quality evidence showing that home-based exercise therapy did not improve walking distance compared to those treated with walking advice (standardised mean difference 0.30; 95% confidence interval -0.45 to 1.05). There is moderate quality evidence that supervised exercise therapy was more effective than home-based exercise therapy in increasing pain-free walking distance at 3 months (standardised mean difference 0.51; 95% confidence interval 0.21 to 0.81), and low quality evidence that it was not more effective in improving quality of life at 3 months (standardised mean difference 0.00; 95% confidence interval -4.79 to 4.79). This review showed moderate and high evidence that supervised exercise therapy provides an important benefit in improving walking distance compared to home-based exercise therapy and walking advice, respectively.
Hageman D, et al. Supervised exercise therapy versus home-based exercise therapy versus walking advice for intermittent claudication. Cochrane Database Syst Rev 2018;Issue 4
Short-term efficacy of minimally invasive treatments for adult obstructive sleep apnea
A systematic review and network meta-analysis was conducted to evaluate the effectiveness of minimally invasive treatments for adult obstructive sleep apnea. The authors included 89 randomised controlled trials (n=6,346) comparing 18 different interventions. The main outcomes were the changes in Apnea-Hypopnea Index and Epworth Sleepiness Scale over 6 months evaluated using weighted mean differences (meta-analysis) and the area under cumulative ranking curves. When compared to no treatment, positive airway pressure was the most effective intervention for reducing the Apnea-Hypopnea Index (weighted mean difference (WMD) 23.3, 95% confidence interval (CI) 19.2 to 27.4), with mandibular advancement devices (WMD 13.29, 95% CI 8.9 to 17.7) and oral negative pressure therapy (WMD 14.10, 95% CI 3.1 to 25.1) ranked second and third (the order was different for the two analysis methods). For reducing the Epworth Sleepiness Scale, the two top-ranking interventions were exercise (WMD 4.25, 95% CI 1.82 to 6.68) and cervico-mandibular support collars (WMD 4.70, 95% CI 0.03 to 9.4), with the ranking being different for the two analysis methods. For both outcomes (Apnea-Hypopnea Index and Epworth Sleepiness Scale), this network meta-analysis concluded that positive airway pressure was the most effective intervention, followed by mandibular advancement devices and positional therapy. While not formally evaluated in this review, complications and side effects associated with the interventions will impact on adherence and long-term treatment success.
Gao Y-N, et al. Short-term efficacy of minimally invasive treatments for adult obstructive sleep apnea: a systematic review and network meta-analysis of randomized controlled trials. J Formos Med Assoc 2019;118(4):750-65
Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease
The aim of this systematic review was to evaluate the efficacy of self-management interventions specifically designed for people with chronic obstructive pulmonary disease (COPD) that include a COPD exacerbation action plan compared with usual care for health-related quality of life, respiratory-related hospital admissions and other health outcomes. Twenty-two studies (n= 3,854 participants) were included in this review. There was a statistically significant effect of self-management interventions with action plans on health-related quality of life over 12 months (mean difference (MD) -2.69, 95% CI -4.49 to -0.90; 1,582 participants; 10 studies; high-quality evidence). Participants in the intervention group were at lower risk for having at least one respiratory-related hospital admission compared with those who received usual care (odds ratio (OR) 0.69, 95% CI 0.51 to 0.94; 3,157 participants; 14 studies; moderate-quality evidence). The number needed to treat to prevent one respiratory-related hospital admission over one year was 12 (95% CI 7 to 69) for participants with high baseline risk and 17 (95% CI 11 to 93) for participants with low baseline risk. There was no difference in the probability of at least one all-cause hospital admission, hospitalisation days, visits to the emergency department or general practitioner, number of COPD exacerbations, all-cause mortality, and dyspnoea scores. To conclude, self-management interventions with a COPD exacerbation action plan improve health-related quality of life and decrease the probability of respiratory-related hospital admissions.
Lenferink A et al. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2017;Issue 8
Exercise-based cardiac rehabilitation in heart transplant recipients
In this new review, the authors included 10 trials (n=300) which evaluated the effects of exercise-based cardiac rehabilitation for people who had received a heart transplantation. Nine studies compared an exercise-only intervention with a no exercise comparator and one study compared high-intensity interval training with moderate-intensity training. Exercise capacity was measured using the peak oxygen uptake (VO2peak). There was moderate quality evidence that exercise-based cardiac rehabilitation improves exercise capacity by 2.49 mL/kg/min of the VO2peak (95% CI 1.63 to 3.36) in people that received heart transplantation compared to those receiving no exercise. However, there was no evidence of a difference between exercise-based cardiac rehabilitation and control groups in four studies. Only one adverse event was reported by one study and it was in the comparator group, not in the intervention group. Exercise-based cardiac rehabilitation did not have an impact on health-related quality of life. Although exercise was effective for improving exercise capacity, more clinical trials with representative samples and high methodological quality are needed to establish the long-term effects of exercise-based rehabilitation in heart transplant recipients.
Anderson et al. Exercise-based cardiac rehabilitation in heart transplant recipients. Cochrane Database Syst Rev 2017;Issue 4
Implementing resistance training in the rehabilitation of coronary heart disease
This review investigated the effectiveness of cardiac rehabilitation consisting of resistance training on outcomes of physical function. Studies including resistance training as a single intervention, or in combination with aerobic training, were included. These were compared to aerobic training alone for cardiorespiratory fitness (VO2 peak and peak work capacity) and muscular strength. Meta-analyses were conducted and the quality of the evidence was classified from very low to high using the GRADE approach. There was moderate quality evidence for improvements in peak oxygen uptake (weighted mean difference (WMD) 0.61 mL/kg/min, 95% confidence internal (CI) 0.20 to 1.10), peak work capacity (standardised mean difference (SMD) 0.38, 95% CI 0.11 to 0.64) and muscular strength (SMD 0.65, 95% CI 0.43 to 0.87) favouring combined training (resistance training in combination with aerobic training). There was no evidence of a difference in effect when comparing resistance training alone to aerobic training, with low quality evidence. Combining resistance training with aerobic training in cardiac rehabilitation is more effective than aerobic training alone for improving physical function.
Xanthos PD et al. Implementing resistance training in the rehabilitation of coronary heart disease: a systematic review and meta-analysis. Int J Cardiol 2017;230:493-508.
Exercise training alone or with the addition of activity counseling improves physical activity levels in COPD
In this recent review, the authors included 37 randomised controlled trials (n= 4,314 participants) that evaluated the efficacy of interventions to improve physical activity levels in people diagnosed with chronic obstructive pulmonary disease (COPD). Primary outcome was physical activity levels and secondary outcomes included exercise capacity, quality of life, dyspnea and lung function. The quality of included studies, according to the PEDro scale, ranged from 3 to 10 points (median [interquartile range] 6 [5 to 7]), where failing to conceal allocation and lack of blinding were the most common methodological limitations in the included studies. Exercise training significantly increased physical activity levels in COPD compared to standard care (standardised mean difference [95% CI] 0.84 [0.44 to 1.25], 3 studies, 103 participants). The addition of activity counselling to pulmonary rehabilitation also increased physical activity levels compared to pulmonary rehabilitation alone (0.47 [0.02 to 0.92], 4 studies, 140 participants). To conclude, exercise training and physical activity counselling were effective strategies to increase physical activity in people with COPD.
Lahham A et al. Exercise training alone or with the addition of activity counseling improves physical activity levels in COPD: a systematic review and meta-analysis of randomized controlled trials. Int J Chron Obstruct Pulmon Dis 2016;11:3121-36
Effect of exercise training on sleep apnea
Eight articles were included in this systematic review (n=180 participants). Six studies were randomised controlled trials and 2 studies were single group intervention studies. Participants’ ages ranged from 32 to 54 years. The studies included both supervised and unsupervised exercise programs in people with obstructive sleep apnea. Treatment programs included a variety of exercise, including aerobic exercise (walking or running), stair climbing, exercise bike, resistance training, and oropharyngeal exercises. Treatment duration ranged from 2 to 6 months, and treatment frequency from 2 to 7 days/week with sessions ranging from 30 to 150 minutes. Control groups included minimal or no intervention. Clinical outcomes were severity of sleep apnea (Apnea Hypopnea Index), body mass index, and patient’s sleepiness (Epworth Sleepiness Scale). Risk of bias for the included studies was measured using the Jadad scale and scores ranged from 1 to 4 (out of 5). Exercise reduced the Apnea Hypopnea Index (standardised mean difference 0.54, 95% confidence interval 0.21 to 0.87, 7 studies) and total Epworth Sleepiness Scale score (standardised mean difference 1.25, 95% confidence interval 0.10 to 2.40, 4 studies) compared to control. There was no statistically significant effect on body mass index (standardised mean difference -0.05, 95% confidence interval -0.04 to 0.28, 4 studies). Exercise therapy was effective for improving clinical outcomes (severity of sleep apnea and patient’s sleepiness) in the treatment of obstructive sleep apnea. The main limitation of this review is the small number of studies and participants included.
Aiello KD, Caughey WG, Nelluri B, Sharma A, Mookadam A, Mookadam M. Effect of exercise training on sleep apnea: a systematic review and meta-analysis. Respir Med 2016;116:85-92.
The effect of early rehabilitation on therapeutic outcomes in ICU patients on mechanical ventilation