Return to all evidence summaries
Continence and women’s health
Continence and women’s health includes, but is not restricted to male and female incontinence and pre- and post-natal interventions for the mother.
The most recently synthesised review is at the top of the list.
- Effectiveness of physical therapy interventions in women with dyspareunia
- Prevention of low back and pelvic girdle pain during pregnancy
- Effects of aerobic exercise performed during pregnancy on hypertension and gestational diabetes
- Motivational strategies to improve adherence to physical activity in breast cancer survivors
- Group-based pelvic floor muscle training for all women during pregnancy is more cost-effective than postnatal training for women with urinary incontinence: cost-effectiveness analysis of a systematic review
- Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women
- Prenatal exercise and cardiorespiratory health and fitness
- Effects of physical exercise after treatment of early breast cancer
- Exercise improves quality of life in patients with cancer
- Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes
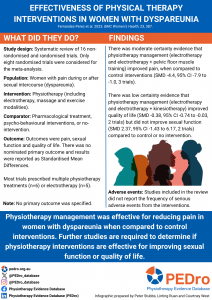
Effectiveness of physical therapy interventions in women with dyspareunia
This systematic review aimed to estimate the effects of physiotherapy compared to pharmacological, psycho-behavioural or no intervention on intensity of perceived pain, sexual function and quality of life in women with dyspareunia.
Five databases were searched from inception to May 2023. Included designs were non-randomised trials, randomised trials and quasi-randomised trials. Studies included women with dyspareunia and compared groups receiving at least one physiotherapy intervention (electrotherapy, massage and exercise modalities) with those receiving pharmacological treatment, psycho-behavioural interventions, or no-intervention. Outcomes of interest were intensity of pain, sexual function and quality of life. Risk of Bias assessment was performed used the ROBINS-I tool for non-randomized trials and the Cochrane Risk of Bias 1 tool for randomized trials. Meta-analyses using random-effects models assessed standardized mean differences (SMD) and 95% confidence intervals (CI). GRADE was applied to each meta-analysis to evaluate the certainty of evidence.
This review included 19 studies; eight randomised trials, two quasi-randomised trials, nine non-randomised studies. Physiotherapy interventions were multiple physiotherapy treatments (n=6), electrotherapy (n=5), pelvic floor muscle training (n=2), Thiele’s massage (n=3), interdisciplinary interventions or pelvic floor muscle training (n=2), extracorporeal shock-wave therapy (n=1). Interventions were 4 weeks to 1 year with at least 1 session per week (when the number of sessions were reported). Only randomised trials were included in the meta-analysis and GRADE synthesis for pain (3 trials, 207 participants), sexual function (2 trials, 373 participants) and quality of life (2 trials, 64 participants).
Compared to control or no intervention, there was moderate certainty evidence that physiotherapy management (electrotherapy and electrotherapy plus pelvic floor muscle training) improved pain (SMD -4.4, 95% CI -7.9 to -1.0). There was low certainty evidence that physiotherapy management (electrotherapy and electrotherapy plus kinesiotherapy) improved quality of life (SMD -0.38 95% CI: -0.74 to -0.03) but did not improve sexual function (SMD 2.37 95% CI: -1.43 to 6.17) compared to control or no intervention. Adverse events were not reported.
The review concluded that physiotherapy was effective for reducing pain in women with dyspareunia when compared to control interventions. Physiotherapy was effective for improving quality of life and ineffective for improving sexual function but there is low certainty evidence. Future research is needed to improve the certainty of the evidence.
Fernandez-Perez P, Leiros-Rodriguez R, Marques-Sanchez MP, Martinez-Fernandez MC, de Carvalho FO, Maciel LYS. Effectiveness of physical therapy interventions in women with dyspareunia: a systematic review and meta-analysis. BMC Womens Health 2023; 23: 387. DOI: doi.org/10.1186/s12905-023-02532-8
Prevention of low back and pelvic girdle pain during pregnancy
During pregnancy, women may experience low back pain (LBP), pelvic girdle pain (PGP) or a combination of both (lumbopelvic pain [LBPP]) which impacts on activities of daily living and their quality of life. Incidence rates are estimated at between 57-90% for LBP and 4-76% for PGP. For women who experience LBP or PGP during pregnancy, up to half will continue to have some pain complaints one year after childbirth.
This systematic review aimed to investigate the short-term and long-term effectiveness and acceptability of a prevention strategy compared to control, on episodes of LBP, PGP or LBPP in women during pregnancy.
Electronic databases were searched from their inception to January 2023. Randomised and quasi-randomised controlled trials enrolling pregnant women without LBP or PGP at the onset of the study were included. Trials needed to compare an experimental group receiving a prevention strategy aimed at preventing LBP, PGP or LBPP during pregnancy to a control group receiving no intervention, placebo, sham or waitlist control. Trials also needed to include at least one of the outcomes of interest, i.e. incidence of LBP, PGP, or LBPP, sick leave and acceptability in the short-term [<12 week] and long-term [> 12 weeks]. Acceptability was measured by the number of participants who withdrew due to any reason out of total number of participants randomly assigned to each group. Risk of bias in each included trial was assessed using the PEDro scale.
Meta-analysis was conducted using a random-effects model, with the reporting of relative risk (RR) and 95% confidence intervals (CI). Trials were grouped by specific prevention strategy, outcome and time points. The GRADE approach was used to rate the certainty of evidence, with the quality of evidence beginning at moderate certainty because it was not possible to assess occurrence of publication bias (small number of trials).
This review included six randomised controlled trials enrolling 2231 pregnant women aged 23-31 years and gestational ages 12-24 weeks. All were low-risk single-child pregnancies and most women were considered sedentary. Eligible trials evaluated two strategies, education combined with exercise and stand-alone exercise. All trials were at a low risk of bias (median PEDro score 7, range 6 to 8). All trials provided data on new events of LBP, PGP or LBPP.
Stand-alone exercise likely reduces the risk of LBP (RR 0.92, 95% CI 0.85–0.99; 2 trials, n=621, moderate certainty evidence), has uncertain effects on reducing the risk of PGP (RR 0.87, 95% CI 0.53–1.44, 1 trial, n=105, very low certainty evidence) and likely does not reduce the risk of LBPP (RR 0.92, 95% CI 0.68–1.25, 2 trials n=1156, moderate certainty evidence) in the long-term. Stand-alone exercise is likely acceptable among women with LBPP (RR 0.60, 95% CI 0.42–0.84, moderate certainty evidence) but uncertain among women with LBP (low certainty evidence).
Education combined with exercise likely does not reduce the risk of LBP or PGP in the short-term (LBP: RR 1.06, 95% CI 0.85–1.31; PGP: RR 1.19, 95% CI 0.71–1.98) or long term (LBP: RR 1.05, 95% CI 0.85–1.30; PGP: RR 1.02, 95% CI 0.80–1.29) (2 trials, n= 438; moderate certainty evidence). There was uncertainty regarding education combined with exercise on LBPP (very low certainty evidence) and no difference between intervention and control groups for acceptability in the short term (very low certainty evidence) and long term (moderate certainty evidence) (2 trials, n=454).
Current moderate quality evidence supports stand-alone exercise as an acceptable intervention for pregnant women with lumbopelvic pain and has a small protective effect regarding episodes of low back pain in the long-term. Further high-quality studies are still required to confirm effects on preventing low back pain, pelvic girdle pain and lumbopelvic pain in the short and long-term.
Santos FF, Lourenço BM, Souza MB, Maia, LB, Oliveira VC, Oliveira MX. Prevention of low back and pelvic girdle pain during pregnancy: a systematic review and meta-analysis of randomised controlled trials with GRADE recommendations. Physiotherapy 118 (2023) 1–11 https://doi.org/10.1016/j.physio.2022.09.004

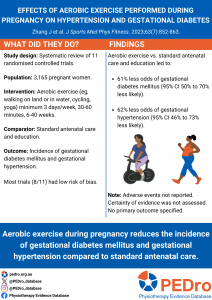
Effects of aerobic exercise performed during pregnancy on hypertension and gestational diabetes
Commonly occurring pregnancy complications include gestational diabetes mellitus and gestational hypertension. Evidence to date regarding the effects of exercise on pregnancy complications and outcomes is inconsistent. This systematic review aimed to estimate the effects of aerobic exercise during pregnancy compared to usual care on gestational diabetes mellitus and gestational hypertension.
Six databases were searched for randomised controlled trials (RCTs). There were no language or date restrictions. Eligible studies included pregnant participants with no history of diabetes, hypertension, psychiatric disorders or underlying disease, including cardiac, kidney, liver or reproductive system diseases. The intervention was any type of aerobic exercise. Usual care participants received standard antenatal care and education. The incidence of gestational diabetes mellitus and gestational hypertension were the outcomes of interest. Data extraction and assessment of methodological quality, using the Cochrane Collaboration Risk of Bias tool, were performed by two authors. Study risk of bias was rated as low (if 4 or more criteria were rated as low), medium (if 2-3 criteria were rated as low) or high (if 0-1 criteria were rated as low). A meta-analysis pooled the trials, with forest plots used to summarise and compare trials. A random effects model was used if significant heterogeneity was found (I2>50%).
Eleven trials, involving 3,165 participants were included. Aerobic exercise predominantly included walking and stationary cycling. Yoga was included in three RCTs and a single trial included aquatic jogging and walking. Intervention frequency was commonly 3 days/week for 30-60 minutes duration and 6-40 weeks. Exercise intensity was poorly reported. The majority of trials (8/11) were rated as having a low risk of bias. Blinding of participants and assessors were the items most frequently associated with a higher risk of bias. A minority of trials (3/11) were also at risk of bias due to unclear randomisation and concealed allocation processes.
The aerobic exercise intervention group showed significant reductions in the incidence of gestational diabetes mellitus compared to usual care (OR=0.39, 95% CI 0.30 to 0.50, I2 0%, p<0.00001, 10 trials). Similarly, the incidence of gestational hypertension was significantly reduced favouring the aerobic exercise group (OR=0.38, 95% CI 0.27 to 0.54, I2 0%, p<0.00001, 9 trials). The incidence of adverse events was not reported.
Aerobic exercise during pregnancy reduces the incidence of gestational diabetes mellitus and gestational hypertension. Further research that allows subgroup analysis of the effects of differing exercise modalities and assessment of evidence certainty is required.
Zhang J, Wang H-P, Wang X-X. Effects of aerobic exercise performed during pregnancy on hypertension and gestational diabetes: a systematic review and meta-analysis. J Sports Med Phys Fitness. 2023 Jul;63(7):852-863. doi: 10.23736/S0022-4707.23.14578-6
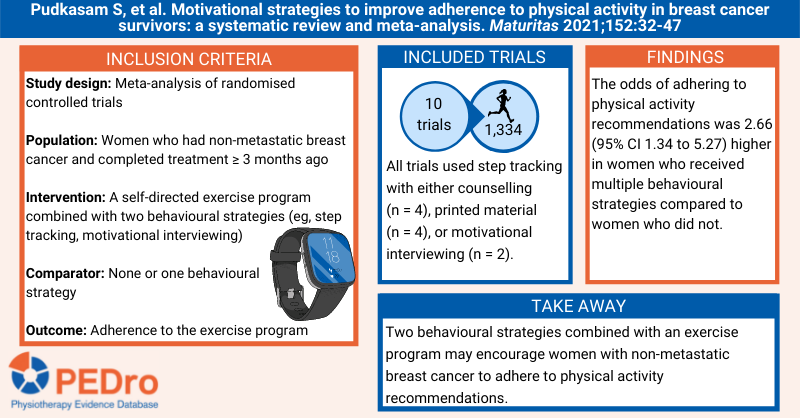
Motivational strategies to improve adherence to physical activity in breast cancer survivors
Breast cancer is the leading cause of cancer morbidity and mortality in women globally. Self-directed physical activity or exercise programs are associated with positive breast cancer outcomes. Behavioural strategies that can increase adherence with these programs include self-monitoring by using a step tracking device and motivational interviewing. This systematic review aimed to estimate the effect of different behavioural strategies to improve adherence to self-directed physical activity or exercise programs in women who had non-metastatic breast cancer.
Guided by a prospectively registered protocol, sensitive searches were performed in six databases (including PubMed and Cochrane CENTRAL) to identify randomised controlled trials evaluating self-directed physical activity or exercise programs in women with non-metastatic breast cancer. Participants must have completed surgery, chemotherapy, and radiotherapy treatments for stage 0 to III breast cancer at least 3 months prior to recruitment. The intervention was any form of self-directed physical activity or exercise program (ie, at least half the program was implemented without supervision from a health professional). Behavioural strategies used in the programs were classified as step tracking and counselling, step tracking and motivational interviewing, and step tracking and printed material. The comparator was usual care. The primary outcome was adherence at the end of follow-up measured as a dichotomous (percentage achieving an exercise volume recommendation – full or partial adherence with the program or a physical activity recommendation) or continuous (measures of exercise duration, intensity, or step count) variable. Two reviewers independently selected trials for inclusion, with any disagreements resolved by a third reviewer. Data were extracted by one reviewer and verified by up to two other reviewers. Two reviewers evaluated risk of bias using the Cochrane risk of bias tool, with any disagreements resolved by discussion. Certainty of evidence was not evaluated. Meta-analysis was used to pool the included trials, using odds ratios and 95% confidence intervals (CI) for dichotomous variables, and standardised mean difference and 95% CIs for continuous variables. Trials in the meta-analysis were grouped according to the behavioural strategies used: step tracking and counselling, step tracking and motivational interviewing, and step tracking and printed material.
Ten trials (1,334 participants) with a follow-up of between 12 weeks and 6 months were included in the meta-analyses. The mean age of women in the trials was 50-62 years. Four trials used step tracking and counselling, two used step tracking and motivational interviewing, and four used step tracking and printed material, in conjunction with a self-directed physical activity or exercise program. Comparator groups received usual care, waitlist control or step tracking.
More participants achieved a physical activity recommendation in groups receiving behavioural strategies in combination with self-directed exercise (218/474, 46%) than in control conditions (152/477, 32%), with an odds ratio 2.66 (95% CI 1.34 to 5.27; 6 trials; 951 participants). This effect was slightly larger for step tracking and counselling (odds ratio 7.10; 95% CI 1.13 to 44.75; 3 trials; 373 participants) and step tracking and motivational interviewing (odds ratio 5.95; 95% CI 2.29 to 15.44; 1 trial; 87 participants) than for step tracking and printed material (odds ratio 1.24; 95% CI 0.72 to 2.13; 2 trials; 491 participants). The outcomes of full or partial adherence with the program were not reported.
Participants in groups receiving behavioural strategies in combination with self-directed exercise achieved 0.55 standard deviations more moderate to vigorous physical activity than those in control conditions (95% CI 0.30 to 0.79; 9 trials; 1,262 participants). This effect was consistent across the step tracking and counselling (standardised mean difference 0.70; 95% CI 0.14 to 1.25; 4 trials; 435 participants), step tracking and motivational interviewing (standardised mean difference 0.70; 95% CI 0.39 to 1.01; 2 trials; 167 participants), and step tracking and printed material (standardised mean difference 0.32; 95% CI 0.07 to 0.57; 3 trials; 660 participants) subgroups.
When combined with a self-directed physical activity or exercise program, the behavioural strategies of step tracking with counselling, motivational interviewing or printed material appear to increase adherence with physical activity in women who had non-metastatic breast cancer.
Pudkasam S, et al. Motivational strategies to improve adherence to physical activity in breast cancer survivors: a systematic review and meta-analysis. Maturitas 2021;152:32-47
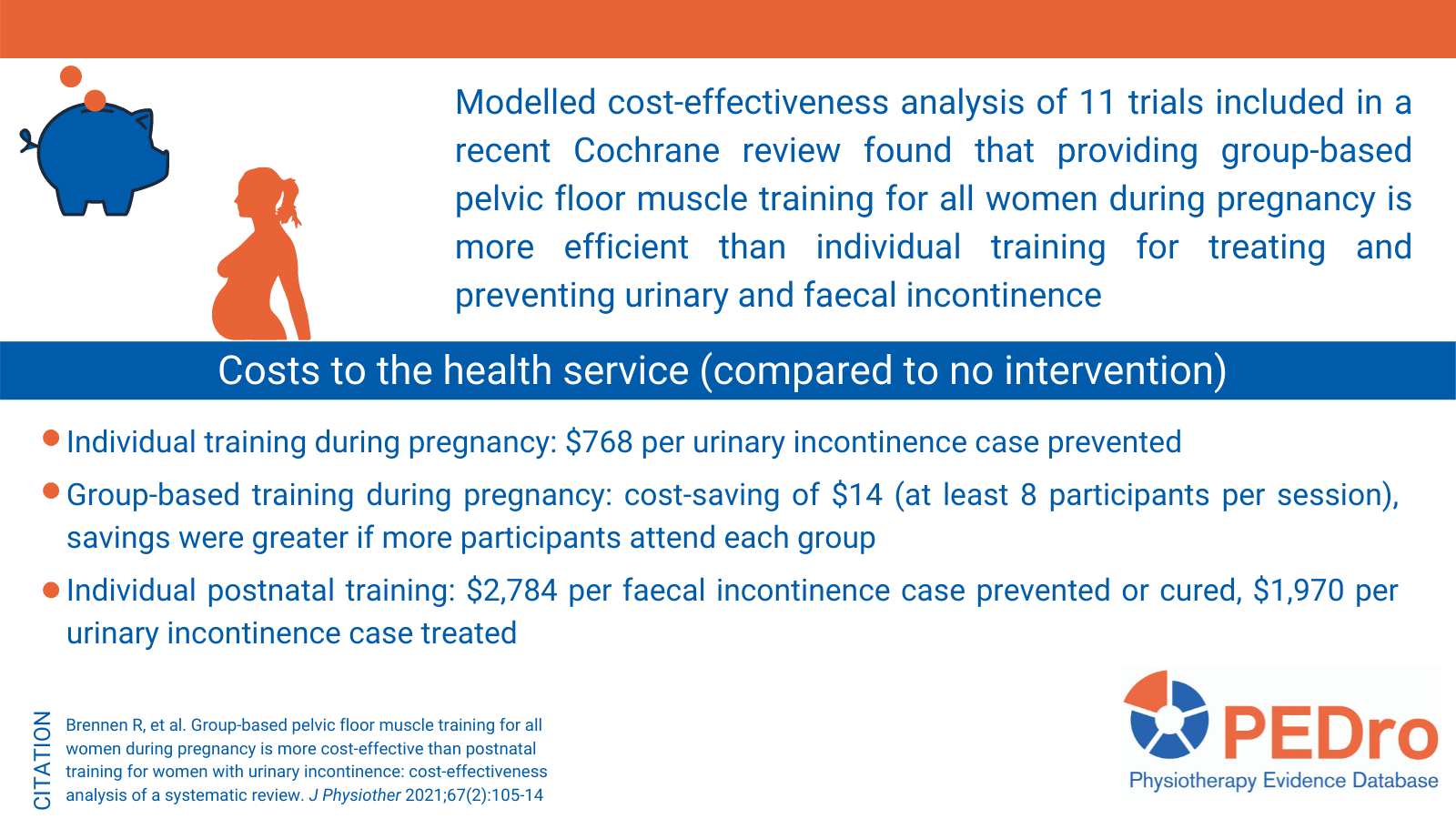
Group-based pelvic floor muscle training for all women during pregnancy is more cost-effective than postnatal training for women with urinary incontinence: cost-effectiveness analysis of a systematic review
Pelvic floor dysfunction and incontinence are common after pregnancy and childbirth. In the first 3 months after childbirth about one in three women have urinary incontinence and up to one in ten have faecal incontinence. Pelvic floor muscle training is the recommended first-line care to prevent and treat both forms of incontinence.
In July 2020 we published a PEDro blog summarising a Cochrane review that estimated the effects of pelvic floor muscle training (antenatal or postnatal) for preventing or treating urinary and faecal incontinence in late pregnancy and after childbirth. The review concluded that structured antenatal pelvic floor muscle training for continent women can prevent the onset of urinary incontinence in late pregnancy and in the early and mid postnatal periods. Uncertainty surrounds the effects of pelvic floor muscle training as a treatment for urinary incontinence in antenatal and postnatal women and for the treatment of faecal incontinence.
Information about value for money is required by health services and policy-makers to inform service planning and determine the best use of the limited funds available to promote health and provide health care. A systematic review has recently been published that expands on the results of the Cochrane review by reanalysing the trials to determine the costs and cost-effectiveness of different models of care used to provide pelvic floor muscle training in the antenatal or postnatal periods. The aim was to determine the most cost-effective way of providing pelvic floor muscle training to prevent or treat postpartum incontinence.
Trials included in the Cochrane review were included in the cost-effectiveness review if they reported statistically significant between-group differences in preventing or curing incontinence and contained sufficient information about the intervention to categorise the pelvic floor muscle training on two strata. The strata were: (1) individual, group-based or mixed individual and group; and (2) during or after pregnancy. The participants were pregnant or postnatal women. The primary outcome was postpartum urinary or faecal incontinence. Costs for each model of intervention were calculated in 2019 Australian dollars using publicly available market rates and enterprise agreements (including estimates of health service, consumer and societal costs plus cost savings). One author performed the calculations, which were cross-checked by a second author. The incremental cost effectiveness of each mode of intervention delivery to successfully prevent or cure one case of incontinence were calculated. Sensitivity analyses were performed to account for variations in the number of participants per group for group-based training, the cost of patient out-of-pocket costs, salary rate of the health professional delivering the intervention and the proportion of patients who would have postnatal incontinence without intervention.
Eleven trials (3,005 participants) were included in the cost effectiveness analysis. Three models of intervention were evaluated: (1) individual pelvic floor muscle training during pregnancy to prevent urinary incontinence (2 trials); (2) group-based training during pregnancy to prevent or treat incontinence (3 trials); and (3) individual postnatal training to treatment urinary incontinence (3 trials) or urinary and faecal incontinence (3 trials).
The costs to the health service to prevent or cure one case of urinary incontinence were $768 for individual pelvic floor muscle training during pregnancy and $1,970 for individual postnatal training. In contrast, group-based training during pregnancy generated a cost saving of $14 if there were eight participants per session. Sensitivity analyses revealed that savings were greater if more participants attend each group. The health service cost per faecal incontinence case prevented or cured was $2,784. The certainty around these cost estimates (ie, 95% confidence intervals) were not reported.
Providing group-based pelvic floor muscle training for all women during pregnancy is more efficient than individual training. However, providing pelvic floor muscle training for postnatal women with urinary incontinence should not be discounted because of the added known benefit for preventing and treating faecal incontinence.
Brennen R, et al. Group-based pelvic floor muscle training for all women during pregnancy is more cost-effective than postnatal training for women with urinary incontinence: cost-effectiveness analysis of a systematic review. J Physiother 2021;67(2):105-14
Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women
Pelvic floor dysfunction and incontinence are common after pregnancy and childbirth. In the first 3 months after childbirth about one-third of women have urinary incontinence and up to one-tenth have faecal incontinence. Pelvic floor muscle training is recommended to prevent and treat incontinence. A recent systematic review aimed to assess the effects of pelvic floor muscle training (antenatal or postnatal) for preventing or treating urinary and faecal incontinence in late pregnancy and after childbirth.
The Cochrane Incontinence Specialised Register was searched to identify randomised or quasi-randomised trials which compared pelvic floor muscle training to no training, usual care, another treatment, or an alternative form of pelvic floor muscle training in pregnant women (could be either continent or incontinent at the time of randomisation). The primary outcome was the self-reported presence of urinary or faecal incontinence. Where possible, risk ratios and 95% CIs were calculated at five time points using meta-analysis: late in pregnancy, in the early (0-3 months), mid (3-6 months) and late (6-12 months) postnatal periods and in the long term (> 5 years). Two reviewers independently selected trials for inclusion, extracted data, and evaluated trial quality. Any disagreements were resolved by discussion. Risk of bias was evaluated using the Cochrane tool and certainty of evidence was evaluated using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. Separate analyses were performed for trials recruiting women who were continent (ie, prevention), women who were incontinent (ie, treatment), mixed prevention and treatment samples, and whether the pelvic floor muscle training occurred before or after delivery. 46 trials (10,832 participants) were included in the analyses.
Prevention of urinary incontinence
Compared with usual care, urinary continent pregnant women performing antenatal pelvic floor muscle training reduced the risk of becoming incontinent in late pregnancy (risk ratio 0.38, 95% CI 0.20 to 0.72, 6 trials, 624 participants, moderate-quality evidence) and in the early (risk ratio 0.38, 95% CI 0.17 to 0.83, 5 trials, 439 participants, GRADE not provided) and mid (risk ratio 0.71, 95% CI 0.54 to 0.95, 5 trials, 673 participants; high-quality evidence) postnatal periods. This effect was not evident in the small number of trials reporting data for the late postnatal period (risk ratio 1.20, 95% CI 0.65 to 2.21, 1 trial, 44 participants, low-quality evidence) and in the long term (risk ratio 1.07, 95% CI 0.77 to 1.48, 2 trials, 352 participants, GRADE not provided).
Treatment of urinary incontinence
Antenatal pelvic floor muscle training in incontinent women did not decrease urinary incontinence in late pregnancy (risk ratio 0.70, 95% CI 0.44 to 1.13, 3 trials, 345 participants, very low-quality evidence) and in the early (risk ratio 0.75, 95% CI 0.37 to 1.53, 2 trials, 292 participants, GRADE not provided), mid (risk ratio 0.94, 95% CI 0.70 to 1.24, 1 trial, 187 participants, low-quality evidence) or late (risk ratio 0.50, 95% CI 0.13 to 1.93, 2 trials, 869 participants, very low-quality evidence) postnatal periods. Pelvic floor muscle training started after delivery for women with urinary incontinence did not reduce the risk of incontinence in the late postnatal period (risk ratio 0.55, 95% CI 0.29 to 1.07, 3 trials, 696 participants, low-quality evidence).
Mixed prevention or treatment of urinary incontinence
Antenatal pelvic floor muscle training in women with or without urinary incontinence (ie, in mixed prevention and treatment samples) probably decreases urinary incontinence in late pregnancy (risk ratio 0.78, 95% CI 0.64 to 0.94, 11 trials, 3,307 participants, moderate-quality evidence) and in the early (risk ratio 0.83, 95% CI 0.71 to 0.99, 6 trials, 806 participants, GRADE not provided) and mid (risk ratio 0.73, 95% CI 0.55 to 0.97, 5 trials, 1,921 participants, low-quality evidence) postnatal periods. This effect was not evident in the late postnatal period (risk ratio 0.85, 95% CI 0.63 to 1.14, 2 trials, 244 women, moderate-quality evidence) or in the long term (risk ratio 1.38, 95% CI 0.77 to 2.45, 1 trial, 188 participants, GRADE not provided). Pelvic floor muscle training started after delivery for mixed prevention and treatment samples did not reduce the risk of incontinence in the late postnatal period (risk ratio 0.88, 95% CI 0.71 to 1.09, 3 trials, 826 participants, moderate-quality evidence).
Faecal incontinence
Only eight trials reported faecal incontinence outcomes. No trials evaluated antenatal pelvic floor muscle training to prevent or treat faecal incontinence. In women in mixed prevention and treatment samples, there was no evidence that antenatal pelvic floor muscle training reduced the risk of faecal incontinence in late pregnancy (risk ratio 0.64, 95% CI 0.36 to 1.14, 3 trials, 910 participants, moderate-quality evidence) or in the early postnatal period (risk ratio 0.76, 95% CI 0.34 to 1.70, 2 trials, 130 participants, GRADE not provided). Pelvic floor muscle training started after delivery for women with incontinence (risk ratio 0.68, 95% CI 0.24 to 1.94, 2 trials, 620 participants, very low-quality evidence) or in mixed prevention and treatment samples (risk ratio 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 participants, low-quality evidence) did not reduce the risk of incontinence in the late postnatal period.
Structured antenatal pelvic floor muscle training for continent women can prevent the onset of urinary incontinence in late pregnancy and in the early and mid postnatal periods. Uncertainty surrounds the effects of pelvic floor muscle training as a treatment for urinary incontinence in antenatal and postnatal women and for the treatment of faecal incontinence.
Woodley SJ, et al. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev 2020;Issue 5
Prenatal exercise and cardiorespiratory health and fitness
Prenatal exercise reduces the serious complications of pregnancy (eg, gestational diabetes, preeclampsia, hypertension) without increasing the risk of having a miscarriage, preterm delivery or low birth weight baby. While pregnant women are encouraged to exercise, the impact of prenatal exercise on cardiorespiratory fitness has not been synthesised. The aim of this systematic review was to assess the effects of prenatal exercise on maternal cardiorespiratory fitness and health compared to not exercising.
Sensitive searches of eight databases were used to locate randomised controlled trials involving pregnant women (at any stage of pregnancy) undertaking an exercise program that started post-conception and lasted for at least 1 week compared to no exercise intervention. The main outcomes were cardiorespiratory fitness (maximal aerobic capacity, submaximal aerobic capacity, aerobic capacity at anaerobic threshold) and cardiorespiratory health (resting heart rate and blood pressure). Two independent reviewers selected trials and extracted the data. Trial quality was evaluated with the Cochrane risk of bias tool and the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) tool was used to determine the certainty of the evidence. Meta-analyses were performed for each outcome and are reported as mean difference (95% confidence interval). Five subgroup analyses were prespecified: (1) with vs. without diabetes; (2) pre-pregnancy body mass index >=25 kg/m2 vs. <25 kg/m2; (3) previously inactive vs. previously active; (4) exercise dose and timing; and, (5) type of test for cardiorespiratory fitness.
26 trials (2,292 participants) were included in the review. Exercise was 2-7 days/week, for 15-60 minutes/session, and started 6-32 weeks into the pregnancy. Exercise modalities included walking, stationary cycling, strength training, aerobics and combined exercises.
There was high certainty evidence that exercise increased absolute maximum aerobic capacity (0.25 L/min (0.11 to 0.39), 3 trials, 77 participants) and relative submaximal aerobic capacity (0.61 mL/kg/min (0.17 to 1.04), 3 trials, 177 participants) compared to not exercising. There was low certainty evidence that exercise increased relative maximal aerobic capacity (2.77 mL/kg/min (0.32 to 5.21), 5 trials, 430 participants) but did not change aerobic capacity at the anaerobic threshold (1.22 mL/kg/min (-0.83 to 3.28), 2 trials, 116 participants). There was high certainty evidence that exercise reduced resting heart rate (-1.7 bpm (-3.2 to -0.2), 9 trials, 637 participants) and low quality evidence that exercise decreased resting systolic blood pressure (-2.1 mmHg (-3.7 to -0.5), 16 trials, 1,672 participants) and resting diastolic blood pressure (-1.8 mmHg (-2.9 to -0.6), 15 trials, 1,624 participants) compared to not exercising.
The subgroup analyses indicated that trials with an exercise duration of <20 weeks had greater reductions in resting diastolic blood pressure than those lasting >20 weeks (-2.9 vs. -0.9 mmHg) and trials that initiated exercise <16 weeks gestational age had smaller reductions in resting diastolic blood pressure than those starting at 16-20 weeks or >20 weeks (-0.9 vs. -2.8 vs. -3.9 mmHg). The other subgroup analyses were inconclusive due to the low number of studies analysed in each category.
Exercise interventions initiated after conception improve maternal cardiorespiratory fitness and health.
Cai C, et al. Prenatal exercise and cardiorespiratory health and fitness: a meta-analysis. Med Sci Sports Exerc 2020 Jan 17:Epub ahead of print
Effects of physical exercise after treatment of early breast cancer
This recent systematic review evaluates the effects of exercise on body composition, quality of life and survival in women after treatment of early-stage breast cancer (stage I to III). Randomised controlled trials evaluating exercise programs after the end of adjuvant treatment were included. Exercise programs could be counselling or structured, supervised or individualised. The primary outcomes were overall survival and disease-free survival. Secondary outcomes were weight loss, body mass index, waist-hip ratio, body fat, and quality of life. The review identified 60 randomised controlled trials (6,303 participants), with structured or individualised exercise being the most common types of exercise evaluated. Only one trial had data for the primary outcomes and suggested that 8 months of exercise reduced overall mortality compared to usual care (hazard ratio 0.45, 95% CI 0.21 to 0.97), but had no effect on disease-free survival (hazard ratio 0.66, 95% CI 0.38 to 1.17). There was low-quality evidence that exercise reduced body mass index (mean difference 0.89kg, 95% CI 0.28 to 1.5) and percentage body fat (mean difference 1.6%, 95% CI 0.88 to 2.31). There was very low-quality evidence that exercise reduced weight (mean difference 1.36kg, 95% CI 0.21 to 2.51), general quality of life (standardised mean difference 0.45, 95% CI 0.2 to 0.69), physical aspects of quality of life (standardised mean difference 0.51, 95% CI 0.23 to 0.79), and mental aspects of quality of life (standardised mean difference 0.28, 95% CI 0.06 to 0.5). This review highlighted the need for more well-designed and large-scale randomised controlled trials to evaluate the effects of exercise on mortality outcomes.
Soares Falcetta F, et al. Effects of physical exercise after treatment of early breast cancer: systematic review and meta-analysis. Breast Cancer Res Treat 2018;170(3):455-76
Exercise improves quality of life in patients with cancer
In this review, the authors included 16 randomised controlled trials examining the effects of exercise during or after chemotherapy and radiotherapy or after surgery compared with placebo, other treatment or standard care. Only studies that used exercise to improve or maintain physical fitness and measured health-related quality of life were included. The review included patients with mixed, breast, lymphoma, colorectal, prostate and lung cancer. Sample sizes ranged from 21 to 269 patients in the included studies. Exercise was effective for improving quality of life among cancer patients when compared to placebo, other treatment or standard care (standardised mean difference 5.6, 95% CI 3.2 to 7.9, 1,735 patients, 16 trials). Benefits of exercise were also evident for secondary outcomes (peak oxygen consumption, self-esteem, physical functioning, fatigue, length of hospital stay, number of general practitioner visits, social functioning). None of the trials included reported adverse events. There is no ideal dosage of exercise therapy for cancer patients; however exercising more frequently and in shorter workouts were associated with better outcomes in the included studies. More studies with long-term follow-ups are needed to investigate the effects of exercise on cancer recurrence and survival rates. Exercise therapy should be recommended during cancer treatment.
Gerritsen JKW, Vincent AJPE. Exercise improves quality of life in patients with cancer: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med 2016;50:796-803.
Read more on PEDro.
Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes
Thirty-six randomised controlled trials were included in this systematic review (n=12,526 women). The mean (SD) age of the participants was 30 years (5.1). The trials included interventions based on diet, physical activity, or a mixed approach of diet, physical activity, and behavior modifying techniques. About 45% of the women included were nulliparous, 40% were obese, and a similar proportion were classified as sedentary. Methodological quality of the included trials was assessed for sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other potential sources of bias. The primary outcomes were gestational weight gain, a composite of maternal outcomes, and a composite of children outcomes. The secondary outcomes were individual maternal and children complications.
For gestational weight gain, the intervention group reported less weight gain than the control group (mean difference (MD) -0.70 kg, 95% confidence interval (CI) -0.92 to -0.48 kg, 33 studies, 9,320 women). Differences in maternal and children composite outcomes were not statistically significant (maternal: odds ratio (OR) 0.90, 95% CI 0.79 to 1.03, 24 studies, 8,852 women; children: OR 0.94, 95% CI 0.83 to 1.08, 18 studies, 7,981 women). For the secondary outcomes, there was strong evidence for a reduction in the odds of caesarean section favouring the intervention group (OR 0.91, 95% CI 0.83 to 0.99, 32 studies, 11,410 women), but not for other individual complications. There is no evidence that effects differ across subgroups of women. In conclusion, diet and physical activity based interventions during pregnancy reduce gestational weight gain and lower the odds of caesarean section.
The International Weight Management in Pregnancy (i-WIP) Collaborative Group. Effect of diet and physical activity based interventions in pregnancy on gestational weight gain and pregnancy outcomes: meta-analysis of individual participant data from randomised trials. BMJ 2017;358:j3119.