Return to all evidence summaries
Gerontology
Gerontology includes papers where the average age of the study sample is over 60, and papers on conditions which commonly affect older people (eg, arthritis).
The most recently synthesised review is at the top of the list.
- Interventions for improving mobility after hip fracture surgery in adults
- Exercise effects on muscle quality in older adults
- Organised inpatient (stroke unit) care for stroke
- Effect of interventions using physical activity trackers on physical activity in people aged 60 years and over
- The added value of therapist communication on the effect of physical therapy treatment in older adults
- Exercise for preventing falls in older people living in the community
- To sit or not to sit? A systematic review and meta-analysis of seated exercise for older adults
- Can exercise improve cognitive symptoms of Alzheimer’s disease?
- Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults
- Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia
- Exercise therapy for functional capacity in chronic diseases
- Exercise to prevent falls in older adults
Interventions for improving mobility after hip fracture surgery in adults
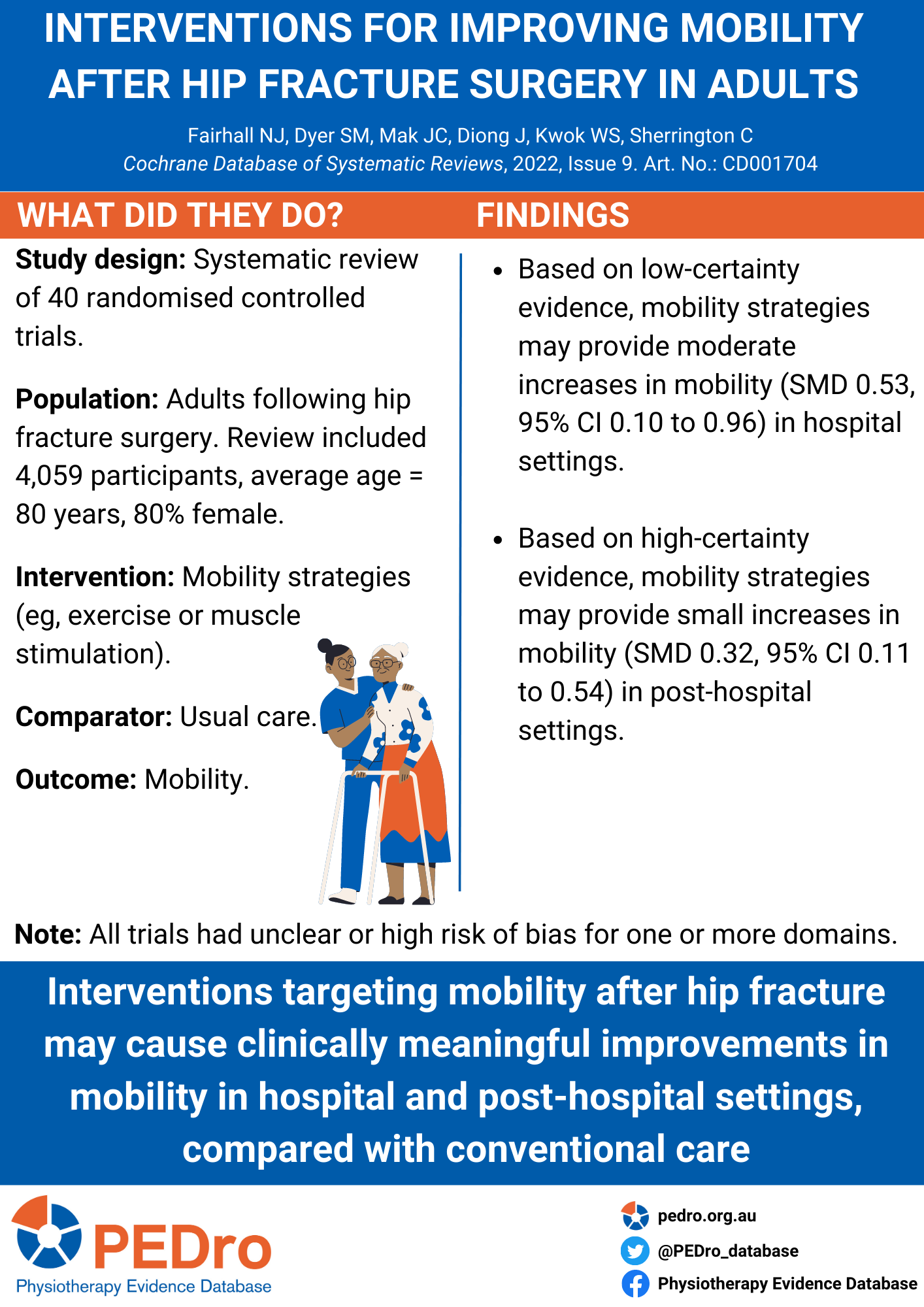
Improving mobility outcomes after hip fracture is key to recovery. Mobility is the ability to move about, including standing up and walking and mobility strategies are treatments that aim to help people move better. This Cochrane systematic review aimed to evaluate the benefits and harms of interventions for improving mobility and physical functioning after hip fracture surgery in adults.
This Cochrane systematic review included randomised controlled trials or quasi-randomised controlled trials that assessed mobility strategies after hip fracture surgery. Eligible trials were identified from 8 electronic databases. Trials were included if they investigated the effect of strategies aimed to improve mobility. These could include care programmes, exercise (gait, balance, functional training, strength/resistance/endurance/flexibility training, three-dimensional exercise and general physical activity) or muscle stimulation. Interventions could be compared to usual care (both in-hospital), no intervention, sham exercise or social visits (post-hospital). Critical outcomes were mobility, walking speed, functioning, health-related quality of life, mortality, adverse effects, and return to living at pre-fracture residence.
Two reviewers identified and selected studies, extracted data, and assessed risk of bias using the Cochrane Risk of Bias 2.0 tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
The review included 40 randomised controlled trials (n = 4059 participants) from 17 countries. Patients were mostly elderly (average age 80 years) and female (80%). All trials had unclear or high risk of bias for one or more domains.
In the hospital setting, there is low certainty evidence that mobility strategies may lead to a moderate, clinically meaningful increase in mobility compared to usual care (standardised mean difference [SMD]: 0.53, 95% confidence interval [CI] 0.10 to 0.96; n = 360). Post-hospital, there is high certainty evidence that mobility strategies compared to usual care, no intervention, sham exercise or social visit led to a small, clinically meaningful increase in mobility (SMD: 0.32, 95% CI 0.11 to 0.54; n= 761). Adverse events were rarely measured by included trials so the safety of these programs in the hospital and out of hospital settings remains unknown.
Compared with conventional care, interventions that target improvement in mobility after hip fracture may improve mobility and walking speed, both in hospital and post-hospital settings. However, long term and economic outcomes have not yet been determined.
Fairhall NJ, Dyer SM, Mak JC, Diong J, Kwok WS, Sherrington C. Interventions for improving mobility after hip fracture surgery in adults. Cochrane Database Syst Rev. 2022 Sep 7;9(9):CD001704.
Exercise effects on muscle quality in older adults
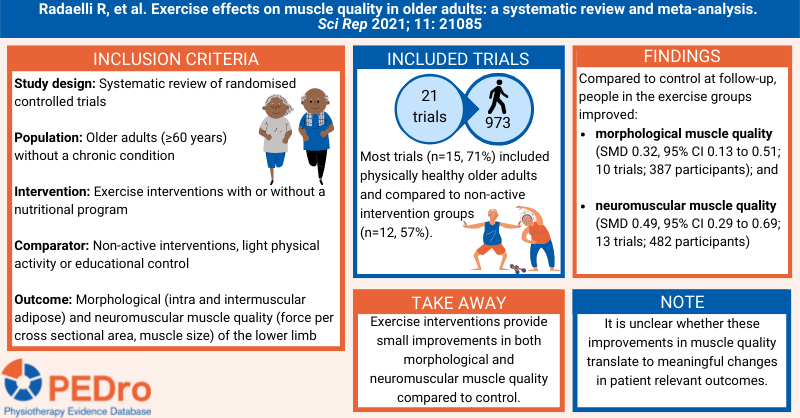
Muscle quality maintenance or improvement is important for older adults to preserve or enhance physical function and metabolic health. There is conflicting evidence on whether exercise interventions improve morphological muscle quality (structure) and neuromuscular muscle quality (strength) in older adults. Further it is unclear which characteristics of exercise and for which populations, lead to greatest change in muscle quality. This systematic review aimed to estimate the effects of exercise interventions compared to non-active control on muscle quality in older adults.
A protocol that was specified a priori guided the methods. Sensitive searches performed in six databases, three grey literature databases, and citation tracking were used to identify randomised controlled trials that were published in English, Portuguese or Spanish. Participants were older adults (≥60 years) without a chronic condition. Interventions were supervised or unsupervised exercise interventions combined or not with nutritional programs. The comparators were mostly non-active interventions, but also included light physical activity (stretching or walking) or an educational control. The primary outcomes were morphological and neuromuscular muscle quality outcomes of the lower limb.
Two independent reviewers selected trials for inclusion, evaluated risk of bias and extracted data. Any disagreements were resolved by consensus discussions or by a third reviewer. Risk of bias was evaluated using the Cochrane risk of bias tool. Certainty of evidence was not evaluated. Meta-analysis was used to pool the included trials to calculate standardised mean differences and 95% confidence intervals (CI). Six subgroup analyses were conducted when data was available; (1) older adults subgroups (e.g., physically healthy, obese, mobility-limited, sarcopenic, frail); (2) exercise delivery modes (e.g., supervised vs. unsupervised exercise programs); (3) intervention modalities (e.g., resistance exercise, aerobic exercise, combined resistance and aerobic exercise, water-based exercise prescription, exercise plus nutritional supplementation); (4) outcomes assessment (e.g., muscle echo intensity, intermuscular adipose tissue); (5) thigh versus calf muscle outcomes (or knee extensors vs. plantar flexors); and (6) based on risk of bias assessment.
21 trials (973 participants) were included in the meta-analyses. Participants had a median age of 70 years (IQR 67-75), were women (n=651, 67%), had a BMI of 27.5 kg/m2 (IQR 25.5–28.4). Most trials (n=15, 71%) included physically healthy older adults and compared to non-active intervention groups (n=12, 57%). Compared to control, participants in the exercise groups had a small improvement in morphological muscle quality (SMD 0.32; 95% CI 0.13 to 0.51; 10 trials; 387 participants) at follow-up. Compared to control, participants in the exercise groups had a small improvement in neuromuscular muscle quality (SMD 0.49; 95% CI 0.29 to 0.69; 13 trials; 482 participants) at follow-up. Both results varied when investigated in subgroup analyses.
Exercise interventions provide small improvements in both morphological and neuromuscular muscle quality compared to control. It is unclear whether these improvements in muscle quality translate to meaningful changes in patient relevant outcomes.
Radaelli, R., Taaffe, D.R., Newton, R.U. et al. Exercise effects on muscle quality in older adults: a systematic review and meta-analysis. Sci Rep 11, 21085 (2021). https://doi.org/10.1038/s41598-021-00600-3
Organised inpatient (stroke unit) care for stroke
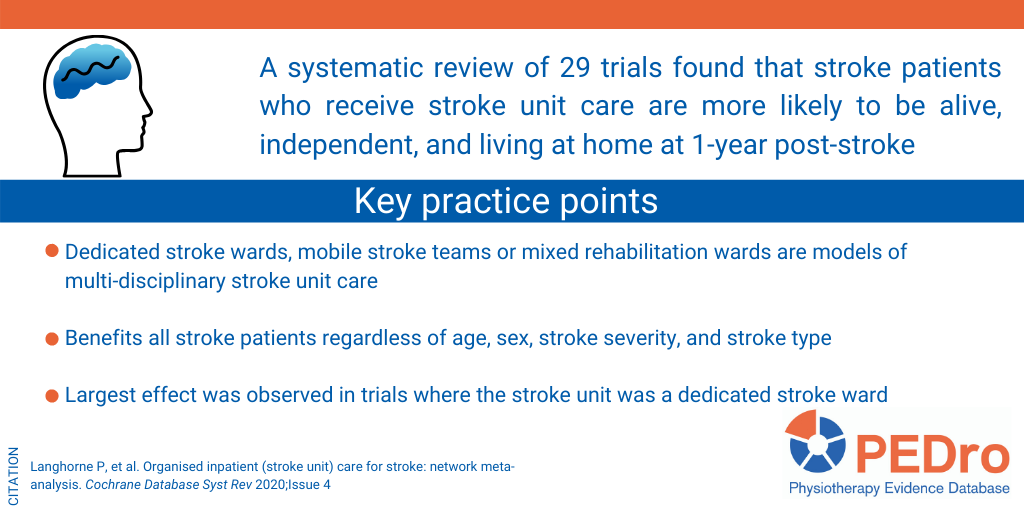
Stroke is the third leading cause of disability and the second leading cause of mortality worldwide. Stroke units provide guideline-directed and multi-disciplinary care (medical, nursing, and allied health, including physiotherapy) for patients hospitalised with stroke. This systematic review aimed to estimate the effect of stroke unit care compared to an alternate form of inpatient care (conventional care or an alternate model of stroke unit care).
The review performed sensitive searches of 13 databases and trial registers (including Medline, Embase, and Cochrane CENTRAL) plus other strategies (including checking reference lists and contacting trialists) to identify randomised controlled trials that compared stroke unit care with an alternate form of inpatient care for people who had sustained a stroke. Pseudo-randomised trials and cross-over trials were excluded. Any model of stroke unit care was included (dedicated stroke ward, mobile stroke team, mixed rehabilitation ward). The comparator was an alternate form of inpatient care, which could include conventional care in a general medical ward or an alternate model of stroke unit care. A clinical definition of stroke was used, and there were no restrictions based on stroke severity or type, age or sex. The composite outcome of death or dependency or requiring institutional care (termed a “poor outcome”) at the end of scheduled follow-up was the primary outcome. One reviewer screened the titles and abstracts of the search results to exclude obviously irrelevant articles. Two reviewers selected trials for inclusion, extracted data, and evaluated risk of bias and certainty of evidence. Risk of bias was evaluated using the Cochrane risk of bias tool. Certainty of evidence was classified using the Grading of Recommendations Assessment, Development and Evaluation (or GRADE) approach. Meta-analysis was used to estimate the risk of a poor outcome, expressed as an odds ratio and its 95% confidence interval (CI). Four subgroup analyses were performed: (1) age <75 years versus 75 years or older; (2) female versus male; (3) mild versus moderate versus severe stroke, and, (4) ischaemic versus haemorrhagic stroke. Network meta-analysis was used to explore the impact of different models of stroke care, with effect size reported as odds ratios and 95% CIs.
29 trials (5,902 participants) were included in the analyses. 20 trials (4,127 participants) compared stroke unit care with conventional care in a general medical ward, 6 trials (982 participants) compared different models of stroke unit care, and 3 trials (793 participants) incorporated more than one comparison.
There was moderate-certainty evidence that stroke unit care reduced the risk of a poor outcome at the end of scheduled follow-up (median 1 year) compared to conventional care, with an odds ratio of 0.77 (95% CI 0.69 to 0.87; 26 trials; 5,336 participants). This outcome was independent of patient age, sex, stroke severity, and stroke type.
The network meta-analysis revealed that this effect was largest when the model of stroke unit care involved a dedicated stroke ward. Using conventional care in a general ward as the comparator, the odds of a poor outcome were 0.74 (95% CI 0.62 to 0.89; moderate certainty) for dedicated stroke wards, 0.88 (95% CI 0.58 to 1.34; low certainty) for mobile stroke teams, and 0.70 (95% CI 0.52 to 0.95; low certainty) for mixed rehabilitation wards.
Stroke patients who receive stroke unit care are more likely to be alive, independent, and living at home 1 year after the stroke. This benefit was independent of patient age, sex, stroke severity and stroke type, and was most obvious in stroke units based in a discrete stroke ward. For every 100 stroke patients receiving stroke unit care, two extra patients will be alive, six more will be independent, and six more living at home.
Langhorne P, et al. Organised inpatient (stroke unit) care for stroke: network meta-analysis. Cochrane Database Syst Rev 2020;Issue 4
Effect of interventions using physical activity trackers on physical activity in people aged 60 years and over
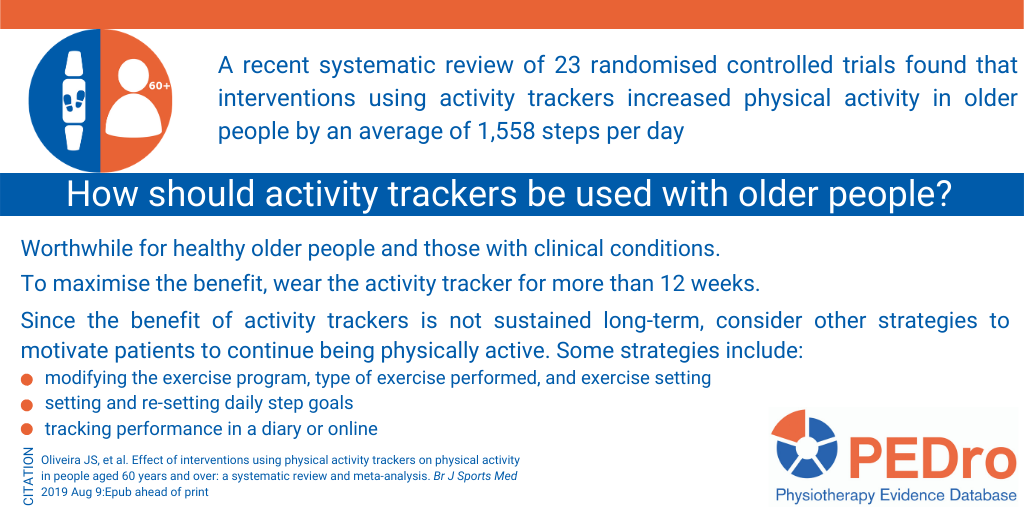
A recent systematic review sought to determine the effect of interventions using activity trackers on physical activity levels and mobility compared with usual care or another physical activity intervention in older people. The review searched eight databases to identify randomised controlled trials involving participants aged 60 years and older. Trials enrolling healthy older adults or older adults with health conditions were eligible. The primary outcome was physical activity quantified as steps per day and measured using an activity tracker or accelerometer. Other types of objective measures of physical activity (e.g., time in moderate-to-vigorous physical activity) or self-reported physical activity measures were excluded. Secondary outcomes included mobility. The methodological quality of the trials was measured with the PEDro scale. The quality of the evidence was assessed with the GRADE approach.
Twenty-three randomised trials including 2,766 participants, with publication dates ranging from 2003 to 2017, were included in the review. There is low quality evidence that participants allocated to activity tracker interventions increased their physical activity levels by 1,558 steps per day (95% confidence interval (CI) 1,099 to 2,018) more than control participants after the intervention. At 12 months post-intervention, the differences between activity tracker and control interventions were not sustained (1 trial, 571 participants; mean difference 210 steps 95% CI -148 to 567). There was moderate quality evidence that activity tracker interventions improved mobility compared to control interventions (3 trials, 218 participants, standardised mean difference 0.61, 95% CI 0.31 to 0.90). Meta-regression did not find any differences in physical activity levels between: trials conducted in healthy populations (9 trials, standardised mean difference 0.61, 95% CI 0.25 to 0.96) versus populations with health conditions (14 trials, standardised mean difference 0.54, 95% CI 0.25 to 0.82)); trials using accelerometers (7 trials, standardised mean difference 0.24; 95% CI -0.15 to 0.63) versus trials using pedometers (16 trials, standardised mean difference 0.69; 95% CI 0.45 to 0.93); or trials with small (< 100 participants) sample sizes (15 trials, standardised mean difference 0.72; 95% CI 0.42 to 1.01) versus large sample sizes (8 trials, standardised mean difference 0.40; 95% CI 0.10 to 0.70). In contrast, a significant interaction between intervention duration and effect size was found, with longer interventions (12 or more weeks) having a larger impact on increasing physical activity levels (18 trials, standardised mean difference 0.70, 95% CI 0.47 to 0.93) compared to shorter interventions (5 trials, standardised mean difference 0.14; 95% CI -0.26 to 0.54). Oliveira JS, et al. Effect of interventions using physical activity trackers on physical activity in people aged 60 years and over: a systematic review and meta-analysis. Br J Sports Med 2019 Aug 9:Epub ahead of print
Read more on PEDro.
The added value of therapist communication on the effect of physical therapy treatment in older adults
This systematic review evaluated whether adding patient-therapist communication during physiotherapy treatment increased self-reported and objectively-measured physical activity levels in older adults. Randomised controlled trials and clinical controlled trials that investigated the effect of adding therapist communication interventions to exercise on physical activity measures, subjective and objective, in older people compared to exercise alone were included.
Outcomes were assessed at the end of the intervention, and up to 12 months after the intervention. The PEDro scale was used to rate risk of bias of the included trials. Self-reported and objectively collected data were analysed as two different outcomes. Meta-analysis was performed when at least three trials were included in a comparison. Altogether, 12 trials were included. Of these, 10 trials included older adults with musculoskeletal conditions, one trial included older people with chronic obstructive pulmonary disease, and one trial included people with stroke.
Objective measures of physical activity were walking speed, timed-up-and-go test, and muscle strength. Self-reported outcomes were motivation to be physically active, confidence to perform exercises, and minutes a day of physical functioning. The frequency of the interventions varied from daily to once per week over a period of 5 days to 9 months. Different behaviour change interventions were used as communication techniques, including credible source, social support, generalisation of the target behaviour, and goals and planning. Overall, communication techniques did not improve performance-based measures of physical activity (standardised mean difference 0.05, 95% CI -0.10 to 0.20), but improved self-reported measures of physical activity (standardised mean difference 0.19, 95% CI 0.07 to 0.31) at the end of the intervention. A similar pattern was observed for the analyses up to 12 months after the end of the intervention – communication techniques did not improve objective measures of physical activity (standardised mean difference 0.00, -0.22 to 0.21), but improved self-reported measures of physical activity (standardised mean difference 0.24, 95%CI 0.05 to 0.44). When interventions were grouped by behaviour change technique, there was no evidence of an effect of social support on objective measures (standardised mean difference -0.02, 95%CI 0.24 to 0.20). The generalisation of target behaviour technique improved self-reported measures of physical activity (standardised mean difference 0.34, 95% CI 0.05 to 0.63). Adding communication techniques based on behaviour change theory to physiotherapy exercise sessions for older people improved self-reported measures of physical activity but not objective measures of physical activity compared to exercise alone.
Lakke S, et al. The added value of therapist communication on the effect of physical therapy treatment in older adults; a systematic review and meta-analysis. Patient Educ Couns 2019;102(2):253-65
Exercise for preventing falls in older people living in the community
A recently published Cochrane review evaluates the benefits and harms of exercise interventions for preventing falls in older people living in the community. This review included randomised controlled trials evaluating any form of exercise as a single intervention in people over 60 years old. The primary outcome was rate of falls (falls per person-year) measured at the time point closest to 18 months post-randomisation. Methodological quality of the included trials was evaluated with the Cochrane risk of bias tool, and the quality of the evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.
This review included 108 trials with 23,407 participants conducted mostly in high income countries. 77% of included participants were women. The average participant age in the included trials was 76 years. Exercise was compared to a control intervention not thought to reduce the rate of falls in people not recently discharged from hospital in 81 trials (n = 19,684 participants) and in people who were recently discharged from hospital in four trials (n = 816 participants). 53% of the interventions included balance and functional exercises as the primary intervention, followed by three-dimensional training (constant repetitive movement through all three spatial planes; 15% of the interventions).
This review found high-quality evidence from 59 trials (n = 12,981 participants) that exercise interventions reduced the rate of falls by 23% (95% CI 17% to 29%) compared to control intervention not thought to reduce falls. There was low-quality evidence from 10 trials (n = 4,047 participants) that exercise interventions reduced the number of people experiencing a fracture following a fall by 27% (95% CI 5% to 44%) compared to control intervention.
Strong evidence shows that exercise interventions reduce the rate of falls in older people living in the community. Further work is needed to understand the impact of resistance training, dance or walking programs. Larger studies are needed to evaluate the impact of exercise on fall-related fractures and falls requiring medical attention.
Listen to Norman Swan interview Cathie Sherrington (Professor from the Institute for Musculoskeletal Health, University of Sydney who is the lead author of the review) for ABC Radio National’s Health Report.
Sherrington C et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev 2019;Issue 1:CD012424
To sit or not to sit? A systematic review and meta-analysis of seated exercise for older adults
This systematic review evaluates the effect of seated exercise on impairment, activity and participation levels of older adults living with a health condition or impairment. This review included trials evaluating seated exercises of various types (eg, resistance, flexibility, range of motion, balance) in people over 65 years of age compared to other exercises or usual care. Methodological quality was evaluated with the PEDro scale, and the quality of evidence of each meta-analysis was assessed using the Grades of Research, Assessment, Development and Evaluation (GRADE) approach. Fourteen trials (n = 921 participants) were included. All outcomes classified by the International Classification of Functioning were considered for this review. The sample was predominantly composed of women. Most studies (n = 9) were considered high quality. Most trials (n = 10) were conducted in residential care facilities or day care centres. The most common intervention was progressive resistance training compared to usual care or social activities. Duration of interventions ranged from six weeks to seven months, with most spanning twelve weeks. Meta-analysis of four trials (n = 141 participants) provided low-quality evidence that seated exercise had a large positive effect on cognition when compared to usual care or social activity (standardised mean difference 1.20, 95% CI 0.25 to 2.16). Meta-analysis of three trials (n = 158 participants) provided moderate quality evidence that seated exercise, compared to social activities, did not have an effect on balance (standardised mean difference 0.13, 95% CI -0.19 to 0.44). Meta-analysis of 3 trials (n = 45 participants) provided low quality evidence that seated exercise did not have an effect on activity as assessed by Timed Up and Go Test (standardised mean difference 0.28, 95% CI -1.08 to 1.63) compared to social activities. In older adults with chronic health conditions, seated exercise was better than usual care to improve cognition, but no better than social activities in improving balance and activity.
Sexton BP, et al. To sit or not to sit? A systematic review and meta-analysis of seated exercise for older adults. Australas J Ageing 2019;38(1):15-27
Can exercise improve cognitive symptoms of Alzheimer’s disease?
In this review, the authors included 19 controlled studies (17 randomised, 1 non-randomised, 1 cross-over) examining the effects of exercise on cognitive function in individuals at risk of or diagnosed with Alzheimer’s disease. Only studies that included an exercise-only intervention compared to a non-diet, non-exercise control group and reported pre- and post-intervention cognitive function measurements were included. The sample (N = 1,150) consisted of older adults (mean age 77, SD 7.5 years), predominantly women (71.1%), who had on average 9.2 (SD 4.3) years of education. Most of the studies included samples of individuals who were at risk of Alzheimer disease because they had mild cognitive impairment (64%; n = 732); another 1% were at risk because they had a parent diagnosed with Alzheimer disease (n = 17), and 35% had diagnosed Alzheimer disease (n = 396). Exercise training was performed, on average, for 3.4 (SD 1.4) days per week at moderate intensity with sessions lasting for 45.2 minutes (SD 17) for 18.6 weeks (SD 10 weeks). Most interventions consisted of aerobic exercise training (65%), with a smaller proportion consisting of a combination of aerobic and resistance training (35%). There was a significant effect of exercise training compared to controls on cognitive function (standardised mean difference (SMD) 0.47, 95% confidence interval (CI) 0.26 to 0.68). For aerobic exercise alone, the between-group effect size was larger (SMD 0.65, 95% CI 0.35 to 0.95). For the combination of aerobic and resistance exercise training the between-group effect size was no longer statistically significant (SMD 0.19, 95% CI -0.06 to 0.43). This meta-analysis provides support for the use of exercise training as a therapeutic modality to improve cognitive function in individuals at risk of or diagnosed with Alzheimer disease. Further studies should investigate physical activity or exercise in combination with other strategies to develop more targeted prevention and treatment options for Alzheimer disease.
Panza GA, et al. Can exercise improve cognitive symptoms of Alzheimer’s disease? J Am Geriatr Soc 2018;66(3):487-95
Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults
This recent systematic review evaluates the effects of physical activity interventions on social functioning, isolation and support in community-dwelling older people. This appears to be the first review to address this question. The protocol for this review was prospectively registered on PROSPERO. The main outcomes were loneliness, social isolation, social support, social networks, and social functioning (a subdomain of health-related quality of life). The review identified 38 randomised controlled trials (5,288 participants) that compared a physical activity intervention to a non-physical activity or control (sedentary) intervention. 26 of the trials had a low risk of bias. A small significant positive effect favouring physical activity intervention was found for social functioning (standardised mean difference 0.30; 95% confidence interval 0.12 to 0.49), but no effect was found for loneliness, social isolation, social support, or social networks. There were sufficient trials to explore the influence of different subgroups on social functioning. The strongest effects were obtained for physical activity interventions provided in isolation, in populations with a medical condition, in the group exercise setting, and when delivered by a medical healthcare provider. Possible mechanisms underlying the social health effects of physical activity are discussed in the article.
Shvedko A, et al. Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: a systematic review and meta-analysis of randomised controlled trials. Psychol Sport Exerc 2018;34:128-137
Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia
In this recent review, the authors included 43 randomised controlled trials (n = 3,988) that evaluated the effects of exercise training on physical function and quality of life in people with cognitive impairment or dementia. Outcomes included strength, flexibility, gait, balance, mobility, walking endurance, dual-task ability, activities of daily living, quality of life, and falls. Trial quality was evaluated using the PEDro scale, with 70% of trials scoring 6/10 or higher. Multimodal exercise (45% of trials) was the most frequently evaluated form of training, followed by aerobic or walking exercise (29%). There was strong evidence that exercise training improved physical function compared to control intervention, with mean between-group differences of 2.1 repetitions (95% CI 0.3 to 3.9) in the 30-second sit-to-stand test, 5cm (95% CI 2 to 8) in step length, 3.6 points (95% CI 0.3 to 7.0) on the Berg Balance Scale, 3.9cm (95% CI 2.2 to 5.5) in functional reach distance, -1 second (95% CI -2 to 0) on the Timed Up and Go test, 0.13m/s (95% CI 0.03 to 0.24) in walking speed, and 50m (95% CI 18 to 81) on the 6-minute walk test. Strong evidence indicated that exercise training did not improve quality of life. The effect of exercise on falls was inconclusive.
Lam FMH, et al. Physical exercise improves strength, balance, mobility, and endurance in people with cognitive impairment and dementia: a systematic review. J Physiother 2018;64(1):4-15
Exercise therapy for functional capacity in chronic diseases
This umbrella review included 85 meta-analyses of randomised controlled trials evaluating the effectiveness of exercise therapy on functional capacity in people with chronic disease. Exercise therapy was compared with no treatment or usual care in adults with non-communicable chronic diseases defined by the World Health Organisation (WHO). The methodological quality of the included meta-analysis was evaluated using the AMSTAR checklist. The type of exercise therapy was classified into four categories: aerobic exercise, resistance training, aerobic and resistance training combined, and other condition-specific exercise-based training. The authors conclude that exercise therapy was effective for improving physical performance and functional capacity in all included chronic diseases (Alzheimer’s disease, cancer, chronic fatigue syndrome, chronic heart failure, chronic kidney disease, chronic obstructive pulmonary disease, cognitive impairment, coronary heart disease, dementia, fibromyalgia, interstitial lung disease, multiple sclerosis, osteoarthritis, Parkinson’s disease, peripheral arterial disease, rheumatoid arthritis, stroke, and type 2 diabetes). Around half of the effect estimates were of moderate to large magnitude and likely to be clinically important. Results were mostly similar among the different types of exercises, except for condition-specific programs that had a lower proportion of significant results compared with the others. Exercise also appears to be safe, but adverse events were not consistently reported. Exercise therapy should be recommended for people with chronic disease to improve functional capacity and reduce disability.
Pasanen T et al. Exercise therapy for functional capacity in chronic diseases: an overview of meta-analyses of randomised controlled trials. Br J Sports Med 2017;51:1459-65
Exercise to prevent falls in older adults
In this updated review, the authors included 88 trials (n=19,478 participants) which tested the effect of exercise to prevent falls in older people. Exercise reduced the rate of falls in community dwelling older people by 21% (pooled rate ratio 0.79, 95% CI 0.73 to 0.85, p<0.001, 69 comparisons). Greater effects were observed with balance training and that least 3 hours per week of exercise (39% reduction in falls). Exercise reduced the rate of falls in people with Parkinson’s disease by 53% (pooled rate ratio 0.47, 95% CI 0.30 to 0.73, p=0.001, 6 comparisons) and by 45% in people with cognitive impairment (pooled rate ratio 0.55, 95% CI 0.37 to 0.83, p=0.004, 3 comparisons). There was no significant effect of exercise for preventing falls in people after stroke (pooled rate ratio 0.74, 95% CI 0.42 to 1.32, p=0.31, 3 comparisons), in people recently discharged from hospital (pooled rate ratio 1.16, 95% CI 0.88 to 1.52, p=0.30, 3 comparisons), and in residential care settings (pooled rate ratio 0.90, 95% CI 0.72 to 1.12, p=0.35, 15 comparisons). Most of the interventions conducted in the included studies involved exercise prescribed as a single intervention by trained health professionals, or professionals specialising in exercise, to minimise the risk of harm during the program. Exercise as a single intervention can prevent falls in community-dwelling older people.
Sherrington C et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med 2017;51(24):1750-8