Return to all evidence summaries
Musculoskeletal
Musculoskeletal includes, but is not restricted to, low back pain, rheumatoid disease, entrapment syndromes, neuralgia.
The most recently synthesised review is at the top of the list.
- Effect of different types of exercise in adult subjects with fibromyalgia
- Exercise effects on muscle quality in older adults
- Effectiveness of pain neurophysiology education on musculoskeletal pain
- Exercise for preventing falls in older people living in the community
- What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines
- Exercise therapy for functional capacity in chronic diseases
General
- The effect of upper cervical mobilization/manipulation on temporomandibular joint pain, maximal mouth opening, and pressure pain thresholds
- The influence of exercise on pain, disability and quality of life in office workers with chronic neck pain
- The effectiveness of physical therapy interventions for athletes post-concussion
- Physiotherapeutic scoliosis-specific exercise for the treatment of adolescent idiopathic scoliosis
- Efficacy of acupuncture for whiplash injury
- Prevention of low back and pelvic girdle pain during pregnancy
- Some types of exercise are more effective than others in people with chronic low back pain
- Exercise therapy for chronic low back pain
- Identification of subgroup effect with an individual participant data meta-analysis of randomised controlled trials of three different types of therapist-delivered care in low back pain
- Prevention strategies to reduce future impact of low back pain
- Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions
- Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain
- Effectiveness of telephone-based interventions for managing osteoarthritis and spinal pain
Spinal
- Shoulder stabilization versus immobilization for first-time anterior shoulder dislocation
- Effectiveness of progressive and resisted and non-progressive or non-resisted exercise in rotator cuff related shoulder pain
Upper limb
- The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery
- Interventions for improving mobility after hip fracture surgery in adults
- Do exercise-based prevention programmes reduce non-contact musculoskeletal injuries in football (soccer)?
- Tai Chi exercise can ameliorate physical and mental health of patients with knee osteoarthritis
- Treatment and prevention of acute and recurrent ankle sprain
- Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players
Lower limb
General
Effect of different types of exercise in adult subjects with fibromyalgia: a systematic review and meta-analysis of randomised clinical trials
Fibromyalgia is a common chronic rheumatic condition associated with widespread musculoskeletal pain and fatigue which impact on mood and health-related quality of life (HRQoL). Low-moderate quality evidence to date has not investigated the efficacy of different types of exercise training. This systematic review aimed to estimate the effects of exercise (aerobic, resistance or stretching) compared to usual care on pain, depression and HRQoL in people with fibromyalgia.
The protocol was prospectively registered. Two databases were searched for randomised controlled trials published in English with no date restriction. Eligible studies included adult participants with fibromyalgia. The intervention was land-based exercise training (aerobic, resistance or stretching). Usual care participants received an alternative exercise type (e.g., aerobic training versus strength training), another type of intervention (e.g., relaxation, chiropractic) or non-exercise usual care. Self-reported pain, depression and HRQoL were the outcomes of interest. Title and abstract, full-text screening for eligibility, data extraction and assessment of methodological quality (using the Cochrane Collaboration Risk of Bias tool) were performed by two authors independently, with disagreements resolved by a third author. A meta-analysis (random effects model) pooled the trials, with forest plots used to summarise and compare trials. Subgroup analyses investigated differences between types of exercise training. Evidence certainty was rated using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach.
Eighteen trials, involving 1,184 (97.5% female) participants were included. Nine trials included aerobic exercise, 10 resistance and five stretching. The intervention parameters varied widely with session duration ranging from 20-60 minutes, frequency from 2-7 days/week and program duration of between three-24 weeks. Risk of bias due to lack of blinding of participants and personnel, blinding of outcomes or incomplete outcomes was high in 14, 2 and 3 trials, respectively.
Four questionnaires were used to report pain, two reported HRQoL and another two depression meaning results were combined as standardised mean differences (SMD) and 95% confidence intervals (CI). All three types of exercise showed significant reductions in pain compared to usual care (SMD=-1.34, 95% CI -1.69 to -0.99, I2 85%, no significant differences between exercise types). Overall exercise showed significant reductions in depression compared to usual care (SMD=-0.78, 95% CI -1.28 to -0.28, I2 85%), subgroup analysis revealed significant effects for aerobic exercise (SMD -0.55 (95% CI -0.97 to -0.12) but not resistance or stretching). Overall exercise showed significant lower impact of fibromyalgia on HRQoL compared to usual care (SMD=-0.95, 95% CI -1.34 to -0.56, I2 82%) and improvements in mental (SMD=0.54 (95% CI 0.23 to 0.84), I2 55%) and physical (SMD=0.80 (95% CI 0.46 to 1.14), I2=62%) components of HRQoL. Adverse events were not reported.
Exercise training for people with fibromyalgia reduces pain and depression and improves HRQoL, although the certainty of available evidence was very low. Further higher-quality evidence is required.
Couto N, Monteiro D, Cid L, Bento T. Effect of different types of exercise in adult subjects with fibromyalgia: a systematic review and meta-analysis of randomised clinical trials. Sci Rep. 2022 Jun 20;12(1):10391. doi: 10.1038/s41598-022-14213-x.

Exercise effects on muscle quality in older adults: a systematic review and meta-analysis
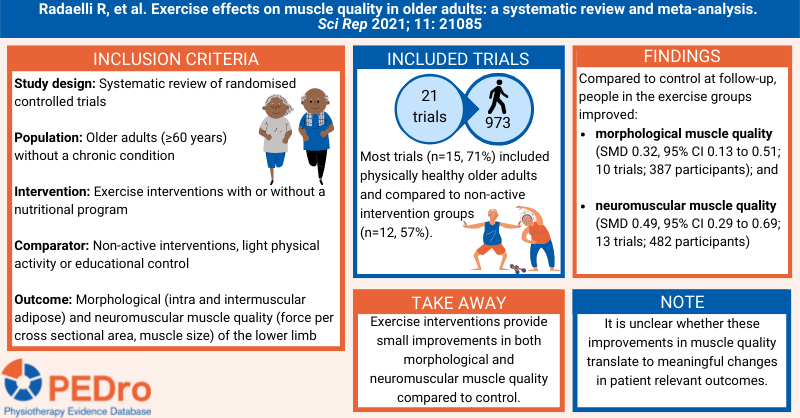
Muscle quality maintenance or improvement is important for older adults to preserve or enhance physical function and metabolic health. There is conflicting evidence on whether exercise interventions improve morphological muscle quality (structure) and neuromuscular muscle quality (strength) in older adults. Further it is unclear which characteristics of exercise and for which populations, lead to greatest change in muscle quality. This systematic review aimed to estimate the effects of exercise interventions compared to non-active control on muscle quality in older adults.
A protocol that was specified a priori guided the methods. Sensitive searches performed in six databases, three grey literature databases, and citation tracking were used to identify randomised controlled trials that were published in English, Portuguese or Spanish. Participants were older adults (≥60 years) without a chronic condition. Interventions were supervised or unsupervised exercise interventions combined or not with nutritional programs. The comparators were mostly non-active interventions, but also included light physical activity (stretching or walking) or an educational control. The primary outcomes were morphological and neuromuscular muscle quality outcomes of the lower limb.
Two independent reviewers selected trials for inclusion, evaluated risk of bias and extracted data. Any disagreements were resolved by consensus discussions or by a third reviewer. Risk of bias was evaluated using the Cochrane risk of bias tool. Certainty of evidence was not evaluated. Meta-analysis was used to pool the included trials to calculate standardised mean differences and 95% confidence intervals (CI). Six subgroup analyses were conducted when data was available; (1) older adults subgroups (e.g., physically healthy, obese, mobility-limited, sarcopenic, frail); (2) exercise delivery modes (e.g., supervised vs. unsupervised exercise programs); (3) intervention modalities (e.g., resistance exercise, aerobic exercise, combined resistance and aerobic exercise, water-based exercise prescription, exercise plus nutritional supplementation); (4) outcomes assessment (e.g., muscle echo intensity, intermuscular adipose tissue); (5) thigh versus calf muscle outcomes (or knee extensors vs. plantar flexors); and (6) based on risk of bias assessment.
21 trials (973 participants) were included in the meta-analyses. Participants had a median age of 70 years (IQR 67-75), were women (n=651, 67%), had a BMI of 27.5 kg/m2 (IQR 25.5–28.4). Most trials (n=15, 71%) included physically healthy older adults and compared to non-active intervention groups (n=12, 57%). Compared to control, participants in the exercise groups had a small improvement in morphological muscle quality (SMD 0.32; 95% CI 0.13 to 0.51; 10 trials; 387 participants) at follow-up. Compared to control, participants in the exercise groups had a small improvement in neuromuscular muscle quality (SMD 0.49; 95% CI 0.29 to 0.69; 13 trials; 482 participants) at follow-up. Both results varied when investigated in subgroup analyses.
Exercise interventions provide small improvements in both morphological and neuromuscular muscle quality compared to control. It is unclear whether these improvements in muscle quality translate to meaningful changes in patient relevant outcomes.
Radaelli, R., Taaffe, D.R., Newton, R.U. et al. Exercise effects on muscle quality in older adults: a systematic review and meta-analysis. Sci Rep 2021; 11, 21085.
Effectiveness of pain neurophysiology education on musculoskeletal pain
Musculoskeletal pain is prevalent, disabling and associated with high socioeconomic costs. In the 2000’s there was a paradigm shift in using education to treat musculoskeletal pain. Traditional education strategies focused on anatomy, biomechanics and the biomedical model for pain (eg, back schools). The contemporary pain neurophysiology (or neuroscience) education model focused on increasing knowledge of pain, the nervous system and the factors modulating pain to reconceptualise pain, including that experiencing pain often relates to hypersensitivity of the nervous system rather than tissue damage. This systematic review aimed to estimate the effects of pain neurophysiology education compared to control on pain, disability and psychological distress in people with musculoskeletal pain.
Guided by a protocol, sensitive searches in seven databases (including Medline, Embase and Cochrane CENTRAL), citation tracking and contacting experts were conducted to identify randomised controlled trials evaluating pain neurophysiology education in people with musculoskeletal pain. Trials recruiting adults with acute or chronic musculoskeletal pain in any body part (spinal or in the extremities) were included. All forms and durations of pain neurophysiology education were accepted (group- or individual-based delivered in person or via other media in isolation or as part of an intervention program). Any intervention or control condition that did not involve pain neurophysiology education could be used as a comparator. The main outcomes were pain intensity, disability and psychological distress (hierarchy of outcomes were Pain Catastrophising Scale, Tampa Scale of Kinesiophobia then other composite scores) measured immediately post-intervention and in the long-term (about 1 year after intervention). Adverse events were also investigated. Two reviewers independently selected trials for inclusion, extracted data and evaluated trial quality and certainty of evidence. Any disagreements were resolved through discussion or by arbitration from a third reviewer. Trial quality was evaluated using the Cochrane risk of bias tool (version 2.0). Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Meta-analysis was used to calculate standardised mean differences and 95% confidence intervals (CI) for between-group differences for each outcome at each time point. The standardised values for pain and disability were transformed to a 0- to 10-point scale by the reviewers. The pre-planned subgroup analyses were acute vs. chronic pain and spinal vs. extremity pain.
18 trials (1,585 participants) were included in the meta-analysis. About 70% of participants were women. The mean age ranged from 37 to 70 years. Three trials recruited people with acute pain and 15 with chronic pain. Participants had spinal pain (10 trials), extremity pain (2), a mix of spinal or extremity pain (1) or other pain conditions (5). Most trials provided individual- or group-based pain neurophysiology education (16 trials) in 1 to 4 sessions lasting 5 to 60 minutes/session. The remaining two trials delivered the intervention as a booklet. The comparator was an alternate form of education (11 trials), usual care (6) or placebo (1).
Mean pain intensity with pain neurophysiology education was lower than control intervention by -0.9 points out of 10 (95% CI -1.7 to -0.1; 11 trials; 944 participants; low certainty) immediately post-intervention and by -1.2 points (-2.3 to -0.1; 10 trials; 903 participants; low certainty) at 1-year. Mean disability with pain neurophysiology education was lower than control intervention by -0.7 points out of 10 (-1.3 to 0.0; 11 trials; 990 participants; low certainty) immediately post-intervention and by -1.0 points (-2.3 to 0.2; 11 trials; 947 participants; low certainty) at 1-year. Mean psychological distress with pain neurophysiology education was -0.36 standard deviations lower than control post-intervention (-0.67 to -0.06; 12 trials; 1,048 participants; low certainty), but the 95% CI for the 1-year estimate included no effect (standardised mean difference -0.37; -0.75 to 0.01; 10 trials; 888 participants; low certainty). There were no adverse events (3 trials).
The pre-planned subgroup analyses revealed no clinically relevant effects for pain intensity, disability and psychological distress immediately post-intervention and at 1-year for participants with acute pain. Standardised mean differences for pain were 0.00 (95% CI -0.19 to 0.19; 2 trials) post-intervention and -0.03 (-0.25 to 0.20; 2 trials) at 1-year. Standardised mean differences for disability were -0.19 (-0.38 to 0.00; 2 trials) post-intervention and 0.01 (-0.33 to 0.35; 2 trials) at 1-year. Standardised mean differences for psychological distress were -0.07 (-0.27 to 0.12; 2 trials) post-intervention and 0.01 (-0.21 to 0.23; 2 trials) at 1-year. In contrast, moderate effects were observed for pain intensity and psychological distress, but not disability, in favour of pain neurophysiology education at post-intervention and 1-year for those with chronic pain. Standardised mean differences for pain were -0.42 (-0.74 to -0.11; 9 trials) post-intervention and -0.52 (-0.97 to -0.06; 8 trials) at 1-year. Standardised mean differences for disability were -0.18 (-0.43 to 0.07; 9 trials) post-intervention and -0.34 (-0.74 to 0.06; 9 trials) at 1-year. Standardised mean difference for psychological distress was -0.46 (-0.83 to -0.08; 10 trials) post-intervention and -0.48 (-0.95 to -0.02; 8 trials) at 1-year. Stratifying by area of pain revealed a tendency for larger effect sizes for spinal pain compared to extremity pain. For example, the standardised mean difference for pain intensity at 1-year was -0.33 (-0.79 to 0.14; 5 trials) for spinal pain and 0.28 (-0.44 to 1.00; 1 trial) for extremity pain.
Pain neurophysiology education may improve pain intensity and psychological distress in people with chronic musculoskeletal pain.
Bulow K, et al. Effectiveness of pain neurophysiology education on musculoskeletal pain: a systematic review and meta-analysis. Pain Med 2021;22(4):891-904
Exercise for preventing falls in older people living in the community
Falls occur in one third of community-dwelling individuals who are more than 65 year of age. Falls can cause serious injuries, and the rate of injuries increase as individuals get older. The aim of this systematic review was to assess the effects of exercise interventions for preventing falls in older people living in the community when compared with a usual care or attention control.
The review included randomised controlled trials that evaluated the effects of exercise interventions compared to usual care or attention control in community-dwelling individuals 60 years of age and older. Exercise programs were classified using the Prevention of Falls Network Europe (ProFaNE) taxonomy (balance and functional exercises, resistance exercises, flexibility, three‐dimensional exercise, walking programmes, endurance, other). The review defined community-dwelling individuals as those living at home or in residences where they do not provide residential health-related care or rehabilitation. The review excluded trials that only included individuals with clinical conditions known to increase the risk of falls, such as Parkinson’s disease, multiple sclerosis, and dementia. The main outcome for this review was the rate of falls. Risk of bias for all eligible trials was assessed using Cochrane’s risk of bias tool. The certainty of evidence was judged using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.
The review included 108 randomised controlled trials, conducted in 25 countries, involving 23,407 participants. 77% of the participants in these trials were women and the average age was 76 years. Overall, there was high-certainty evidence that exercise reduced the rate of falls by 23% when compared to control (rate ratio 0.77, 95% confidence interval (CI) 0.71 to 0.83, 59 trials, 12,981 participants). Certain exercise types reduced the rate of falls more than others when compared to control, there was: high-certainty evidence for interventions that mainly focussed on balance and functional tasks (rate ratio 0.76, 95% CI 0.70 to 0.81, 39 trials, 7,920 participants); moderate-certainty evidence for balance and functional exercises with resistance exercises (rate ratio 0.66, 95% CI 0.50 to 0.88, 11 trials, 1,374 participants); and, low-certainty evidence for three-dimensional exercise (Tai Chi or similar) (rate ratio 0.81, 95% CI 0.67 to 0.99, 7 trials, 2,655 participants).
Subgroup analyses showed that there was little difference in the effect of exercise on the rate of falling when:
- trials included participants at increased baseline risk of falling compared to trials that did not (rate ratio 0.80, 95% CI 0.72 to 0.88 versus 0.74, 95% CI 0.65 to 0.84)
- trials that only included participants 75 years of age and older compared to trials of participants less than 75 years of age (rate ratio 0.83, 95% CI 0.72 to 0.97 versus 0.75, 95% CI 0.69 to 0.82)
- trials where the exercise intervention was delivered in a group setting compared to individually delivered exercise (rate ratio 0.76, 95% CI 0.69 to 0.85 versus 0.79, 95% CI 0.71 to 0.88).
- Exercise interventions led by health professionals (such as a physiotherapist) resulted in a greater reduction in the rate of falls compared to those led by non-health professionals (such as a trained fitness leader), although both still resulted in a reduction in rate of falls (rate ratio 0.69, 95% CI 0.61 to 0.79 versus 0.82, 95% CI 0.75 to 0.90).
There is high-certainty evidence that exercise interventions reduce the rate of falls by 23% in community dwelling individuals aged over 60 years of age compared to control. If there were 850 falls in 1,000 people followed over 1 year, exercise would result in 195 fewer falls (95% CI 144 to 246). Exercise interventions that primarily focus on balance and functional activities can reduce the rate of falls. Exercise led by health professionals result in a greater reduction in the rate of falls.
Sherrington C et al. Exercise for preventing falls in older people living in the community: an abridged Cochrane systematic review. Br J Sports Med 2020;54(15):885-91
What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines
This systematic review evaluated recommendations for high-quality care for common musculoskeletal pain sites treated in emergency departments and primary care. Evidence-based clinical practice guidelines for adult musculoskeletal pain that were written in English and published since 2011 were included. Guidelines were excluded if they focussed on traumatic musculoskeletal pain, single modalities (eg, surgery), traditional medicine, and specific disease processes. Quality was evaluated using the Appraisal of Guidelines for Research and Evaluation II (AGREE-II) instrument. Guidelines scoring at least 50% in the rigour of development, editorial independence, and stakeholder involvement domains were included in the analyses. Recommendations from the included guidelines were extracted and coded.
There were 11 high-quality guidelines focussing on low back (n = 4), hip or knee (n = 4), neck (n = 2) and shoulder (n = 1) pain. These guidelines contained 11 consistent recommendations that can be used by healthcare consumers, clinicians, researchers and policy makers to improve the quality of care for musculoskeletal pain. The recommendations are:
- Ensure care is patient centred
- Screen for red flag conditions
- Assess psychosocial factors
- Use imaging selectively
- Undertake a physical examination
- Monitor patient progress
- Provide education or information
- Address physical activity or exercise
- Use manual therapy only as an adjunct to other treatments
- Offer high-quality non-surgical care prior to surgery
- Try to keep patients at work.
A great infographic summarising these recommendations has been produced by the British Journal of Sports Medicine.
Lin I et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med 2020;54(2):79-86

Exercise therapy for functional capacity in chronic diseases
This umbrella review included 85 meta-analyses of randomised controlled trials evaluating the effectiveness of exercise therapy on functional capacity in people with chronic disease. Exercise therapy was compared with no treatment or usual care in adults with non-communicable chronic diseases defined by the World Health Organisation (WHO). The methodological quality of the included meta-analysis was evaluated using the AMSTAR checklist. The type of exercise therapy was classified into four categories: aerobic exercise, resistance training, aerobic and resistance training combined, and other condition-specific exercise-based training. The authors conclude that exercise therapy was effective for improving physical performance and functional capacity in all included chronic diseases (Alzheimer’s disease, cancer, chronic fatigue syndrome, chronic heart failure, chronic kidney disease, chronic obstructive pulmonary disease, cognitive impairment, coronary heart disease, dementia, fibromyalgia, interstitial lung disease, multiple sclerosis, osteoarthritis, Parkinson’s disease, peripheral arterial disease, rheumatoid arthritis, stroke, and type 2 diabetes). Around half of the effect estimates were of moderate to large magnitude and likely to be clinically important. Results were mostly similar among the different types of exercises, except for condition-specific programs that had a lower proportion of significant results compared with the others. Exercise also appears to be safe, but adverse events were not consistently reported. Exercise therapy should be recommended for people with chronic disease to improve functional capacity and reduce disability.
Pasanen T et al. Exercise therapy for functional capacity in chronic diseases: an overview of meta-analyses of randomised controlled trials. Br J Sports Med 2017;51:1459-65
Spinal
The effect of upper cervical mobilization/manipulation on temporomandibular joint pain, maximal mouth opening, and pressure pain thresholds
This systematic review aimed to explore the effects of upper cervical (C0/1, C1/2, or C2/3) mobilization/manipulation compared to sham or other inventions on pain, mouth opening and pressure pain thresholds in adults with temporomandibular joint (TMJ) dysfunction.
Four databases including Medline, CINAHL, EMBASE and The Cochrane Library were searched for randomised controlled trials (RCTs) published in English or translated using Google Translate into English. Eligible studies included people aged ≥ 18 years with TMJ pain of insidious onset and interventions utilising articular joint mobilizations and/or manipulations to the upper cervical spine compared to sham or other intervention. Outcome measures were pain on a visual analogue scale (VAS) or numeric pain rating scale (NPRS), maximal mouth opening (MMO) measured in millimetres using a range of motion (ROM) scale, and pressure pain threshold (PPT) of the temporalis and masseter muscles measured in kg/cm2 using a pressure algometer. Full text articles were independently screened by two reviewers with disagreements resolved through discussion. Minimal clinically important differences of a change of 2.0 points on the NPRS or VAS, 2.5mm for MMO, and 0.2kg/cm2 for the masticatory muscles. Authors were contacted to obtain insufficient or missing data. Risk of bias was independently evaluated by two reviewers using the Cochrane Risk of Bias Tool and resolved through discussion. Evidence quality and strength of recommendations for outcomes was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system. A random-effects meta-analysis was conducted . Adverse events were not reported in the review.
Eight studies involving 437 participants were included. Four studies compared mobilization/manipulation with no intervention, three studies compared mobilization/manipulation with another intervention, and one study had multiple comparison groups. The average age of participants ranged from 20 to 47 years. Five trials included men and women, three included women only. The duration of TMJ symptoms was not stated in two trials, greater than one month in one trial, greater than three months in three trials, at least six months in one trial and between one and five years in one trial. Pain was measured in five trials, MMO in six trials, PPT of the masseter in four and of the temporalis in five trials. Treatment ranged from one to ten sessions and outcomes were assessed immediately after treatment to 32 weeks post-treatment. Of the included trials, one had low risk of bias, five has unclear risk of bias and two had high risk of bias.
Meta-analysis showed that mobilization/manipulation: reduced pain intensity compared to sham (MD = -1.93, 95% CI-3.61 to -0.24, n = 93, 2 trials, I2 = 83%) and compared to other interventions (MD = -1.03, 95% CI -1.73 to -0.33, n = 137, 3 trials, I2 = 27%); increased MMO compared to sham (MD = 2.11mm, 95% CI 0.26 to 3.96, n = 123, 3 trials, I2 = 0%) and compared to other interventions (MD = 2.25mm, 95% CI 1.01 to 3.48, n = 198, 4 trials, I2 = 0%). Mobilization/manipulation did not demonstrate a minimal clinically important difference for pain intensity nor MMO. Meta-analysis did not reveal an improvement in PPT for the masseter or temporalis muscles when comparing mobilization/manipulation to sham or other interventions. Using the GRADE approach, the certainty of evidence was moderate for pain and MMO, and low for PPT for the masticatory muscles.
Due to the low-moderate certainty evidence, a small number of trials, heterogeneity of included trials, and imprecise treatment estimates, it is unclear whether upper cervical spine mobilization/manipulation provides meaningful improvement in pain intensity, mouth opening, and pressure pain threshold in individuals with TMJ dysfunction.
Lam AC, Liddle LJ, MacLellan CL. The effect of upper cervical mobilization/manipulation on temporomandibular joint pain, maximal mouth opening, and pressure pain thresholds: a systematic review and meta-analysis. Archives of Rehabilitation Research and Clinical Translation 2023 Nov;5(1):100242

The influence of exercise on pain, disability and quality of life in office workers with chronic neck pain
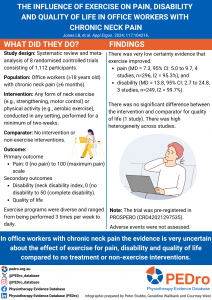
Systematic review found that in office workers with chronic neck pain there is very low certainty evidence that exercise improves neck pain and disability compared to no intervention.
Systematic review found that in office workers with chronic neck pain there is very low certainty evidence that strengthening exercise improves neck pain and disability compared to no intervention.
Neck pain is a common in people in ‘office workers’ working in offices or at home. A previous systematic review showed that exercise reduced pain but there was significant heterogeneity between studies, with many studies having low sample sizes. This systematic review is an update of the evidence. The review aimed to estimate the effects of exercise compared to any non-exercise comparator on pain (primary outcome), disability and quality of life (secondary outcomes) in office workers with chronic neck pain.
Ten databases were searched for randomised controlled trials (RCTs) published in English. Eligible studies included people aged ≥18 years, with self-reported chronic neck pain (lasting ≥6 months) who are currently working in an office-based occupation. Excluded studies were any diagnosis of spinal pathology (e.g., radiculopathy, whiplash, tumour, fracture, dislocation, infection, or systemic disease). The intervention was any form of neck exercise (e.g., strengthening, motor control) or physical activity (e.g., aerobic exercise), conducted in any setting, performed for a minimum of two-weeks without any other additional treatment besides advice or education. The comparator was no intervention or any non-exercise training intervention. The outcomes were neck pain intensity (primary outcome), disability and quality of life (secondary outcomes). Study selection, data extraction and assessment of Risk of Bias, using the Cochrane Risk of Bias 2.0 tool, were performed by two authors. For each outcome, trials were pooled in a meta-analysis using a random effects model, using forest plots. Certainty of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system.
Eight studies, involving 1112 participants were included. Studies were from Denmark (n=2), China (n=2), Finland (n=2), Thailand (n=1) and South Korea (n=1). The workplace included people working in office buildings (n=3), university admin staff (n=2), occupational healthcare centres (n=2) and elementary school workers (n=1). Exercise programs were diverse (including progressive resistance training, scapular function training, endurance training, thoracic extension exercises, and exercises with biofeedback) and ranged from being performed 3 times per week to daily, with a treatment duration from 4 to 12 weeks. All studies were judged to have high risk of bias.
All studies included in the meta-analysis and GRADE synthesis compared exercise to no training. Heterogeneity across the studies was significantly high. There was very low certainty evidence that exercise improved pain intensity (MD = 7.3, 95% CI 5.0 to 9.7, 4 studies, n=296, I2 = 95.3%) and disability (neck disability index) (MD = 13.8, 95% CI 2.7 to 24.8, 3 studies, n=249, I2 = 99.7%). One study assessed quality of life, and no meta-analysis was performed. The study found no significant difference in quality of life for strengthening exercises.
In office workers with chronic neck pain the evidence is very uncertain about the effect of exercise for pain, disability and quality of life compared to no treatment or no exercise.
Jones LB, Jadhakhan F, Falla D. The influence of exercise on pain, disability and quality of life in office workers with chronic neck pain: A systematic review and meta-analysis. Appl Ergon. 2024: 117: 104216. doi: 10.1016/j.apergo.2023.104216
The Effectiveness of physical therapy interventions for athletes post-concussion
This systematic review aimed to investigate the effects of physical therapy interventions compared to alternative treatments in adolescent and young adult athletes post-concussion.
Articles were included if they were randomized controlled-trials, had participants who were athletes under the age of thirty who had an acute or chronic sport-related concussion, and the intervention was physical therapy, including aerobic and multimodal interventions. Six databases were searched between March 2021 and January 2022. The PEDro scale was used to assess methodological quality of included trials to indicate high (>5/10), moderate (5/10) and low (<5/10) quality.
Eight articles were included in the review. Four assessed aerobic intervention and four assessed multimodal intervention. Multimodal treatment included individualised exercise progression, early intervention, cervical spine and vestibular rehabilitation, asymptomatic exercise and visualisation and imagery. Control treatment included stretching, education, subtherapeutic exercise, range of motion exercise, visualisation, rest and delayed intervention.
The outcome measures included the days from injury to recovery, PCSS, PCSI, Health Related Quality of Life, Beck Depression Inventory for Youth, Pediatric Quality of Life Multidimensional Fatigue Scale, the BESS, ImPACT, time to return to play, health and demographic questionnaires, Borg CR10, Rate of Perceived Exertion (RPE), and Post Ride Symptom Change Rating. The control groups either participated in education, rest, sub-therapeutic exercise, placebo, or sham treatment. None of the studies demonstrated any significant adverse effects from early physical activity and physical therapy intervention.
375 athletes (163 females and 212 males) participated in the eight studies with ages ranging from 11.2 to 21.2 years. The severity of symptoms ranged from acute post-concussion symptoms to chronic post-concussion symptoms. One article did not indicate the severity of concussion. Participants had either one concussion or a recurrence of concussions. Two articles did not indicate the occurrence of concussion.
Five of the eight articles were of a higher quality relating to risk of bias compared to the other three included articles, with scores ranging from a 5 to a 10 out of 10 points although there is no indication that the assessor had undertaken PEDro reviewer training.
Three of the five higher-quality articles found significant improvements in the treatment groups compared to the control groups with reduction in symptoms and time to recovery. All articles demonstrated improved symptoms with time and no notable adverse effects were reported with early physical activity and therapy. Due to the variability in the types of intervention utilised and the subjects on whom the interventions and controls were performed, the study was unable to determine the optimal treatment intervention.
This systematic review suggests that aerobic exercise or multi-modal interventions may lead to quicker recovery and return to sport in adolescent and young adult athletes with post-concussive symptoms when compared to traditional treatments such as physical and cognitive rest.
Art K, Ridenour C, Durbin S, Bauer M, Hassen-Miller A. The Effectiveness of physical therapy interventions for athletes post-concussion: a systematic review. Int J Sports Phys Ther. 2023 Feb 1;18(1):26-38.

Physiotherapeutic scoliosis-specific exercise for the treatment of adolescent idiopathic scoliosis
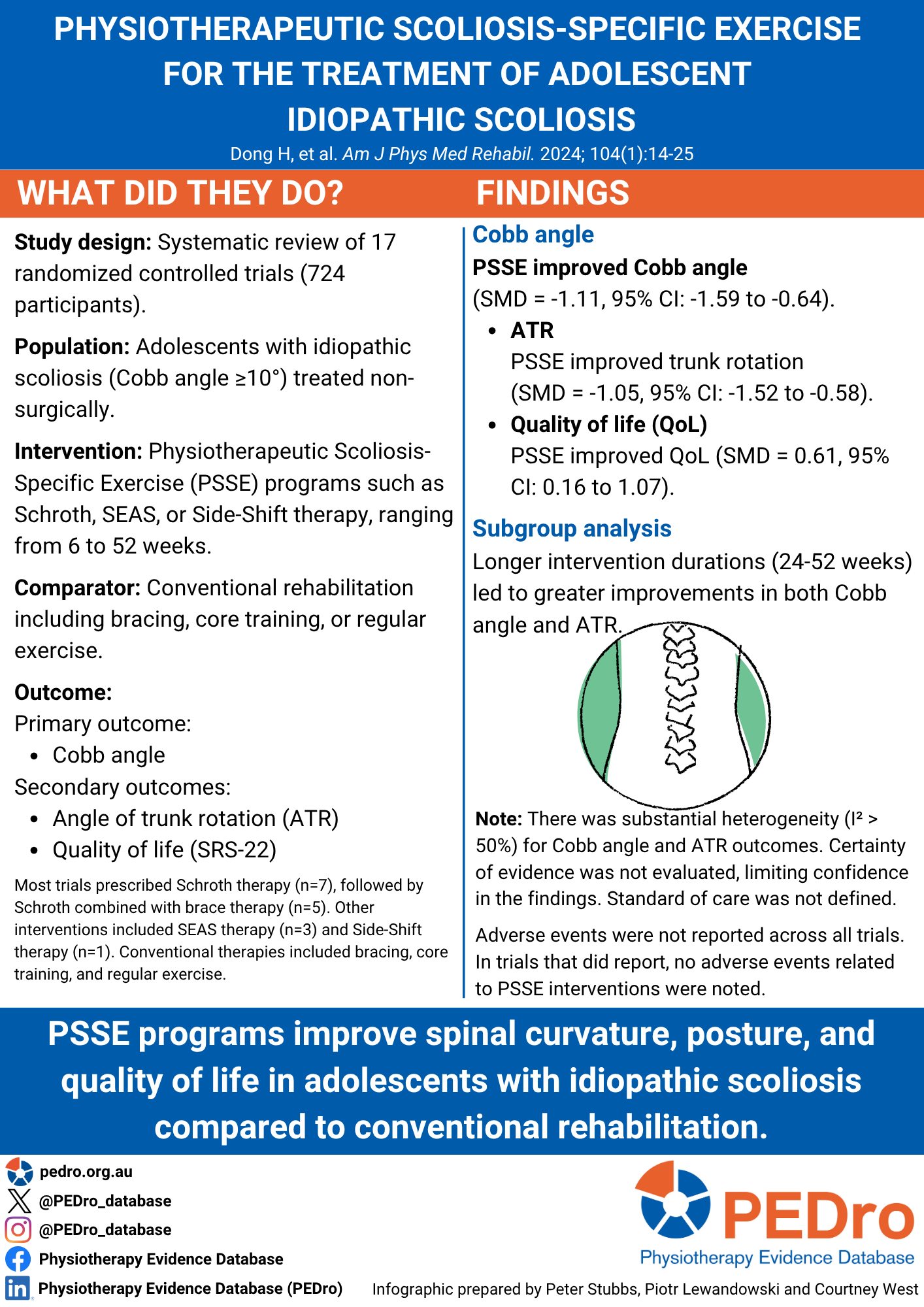
Idiopathic scoliosis is a S-shaped curvature of the spine, defined as having a Cobb angle of 10 degrees or more. Without treatment, progressive spinal deformities can limit cardiorespiratory function, coordination, balance, and quality of life. Non-surgical approaches to adolescent idiopathic scoliosis include conventional rehabilitation (eg. braces, and standard care ) or physiotherapy scoliosis-specific exercise (PSSE) . PSSE includes Schroth therapy, Scientific Exercise Approach to Scoliosis (SEAS) therapy, and Side-Shift Therapy. This systematic review aimed to determine the efficacy of PSEE in improving the Cobb angle in adolescents with idiopathic scoliosis compared to conventional rehabilitation.
Eight databases were searched for randomised controlled trials (RCTs) published in English and Chinese. Studies with poor methodological quality or incomplete data were excluded. Eligible studies included adolescents diagnosed with idiopathic scoliosis according to the 2016 SOSORT guidelines. The intervention was any PSSE-based rehabilitation such as Schroth, SEAS, BSPTS, Dobomed, Side Shift, FITS, and Lyon. The comparator was any conventional rehabilitation including brace therapy, core training, regular exercise, proprioceptive neuromuscular facilitation, or standard care. The Cobb angle was the primary outcome of interest with secondary outcomes include angle of trunk rotation (ATR) and quality of life, as measured by the Scoliosis Research Society – 22 item questionnaire (SRS-22). Study selection and assessment of methodological quality, using the Cochrane Risk of Bias Tool, were performed by two authors. Evidence certainty was not assessed. A meta-analysis pooled the trials, with forest plots used to summarise and compare trials. A random effects model was used if significant heterogeneity was found (I2>50%).
Seventeen trials, involving 724 participants, were included. Trials investigated five types of PSSE therapies: Schroth combined with SEAS therapy (n=1), Schroth combined with brace therapy (5 trials), Schroth alone (7 trials), SEAS alone (3 trials), or Side-Shift therapy (1 trial). Interventions ranged from 30-90 minutes per session, 1-7 days a week for 6-52 weeks. Conventional therapies included bracing (7 trials), standard care (6 trials), core training (2 trials), PNF (1 trial), or regular training (1 trial). Unclear or high risk of bias was due to lack of concealed allocation (11 trials); blinding of participants or personnel (11 trials); blinding of outcome assessors (9 trials); and selective reporting bias (9 trials ). The frequency of adverse events was not reported in the systematic review.
Compared to conventional rehabilitation, PSSE therapies improved Cobb angle (SMD = -1.11, 95% CI: -1.59 to -0.64, n = 724, 17 trials, I2= 89%); ATR (SMD = -1.05, 95% CI: -1.52 to -0.58, n = 622, 13 trials, I2= 85%); quality of life (SMD = 0.61, 95% CI: 0.16 to 1.07, n = 333, 7 trials, I2= 74%). Amount of improvement in Cobb angle differed by intervention duration: 6-24 weeks (SMD = -0.77, 95% CI: -1.11 to -0.43, n = 150, 5 trials, I2= 1%); 24-52 weeks (SMD = -1.04, 95% CI: -1.29 to -0.79, n = 287, 6 trials, I2= 7%). Amount of improvement in ATR also differed by intervention duration: 6-24 weeks (SMD = -0.37, 95% CI: -0.7 to -0.04, n = 150, 5 trials, I2= 0%); 24-52 weeks (SMD = -1.53, 95% CI: -2.22 to -0.84, n = 472, 8 trials, I2= 89%).
PSSE therapies may improve body posture, trunk rotation, and quality of life in adolescents with idiopathic scoliosis compared to conventional rehabilitation.
Dong H, You M, Li Y, Wang B, Huang H. Physiotherapeutic Scoliosis-Specific Exercise for the treatment of adolescent idiopathic scoliosis: A systematic review and network meta-analysis. Am J Phys Med Rehabil. Published online May 10, 2024. doi:10.1097/PHM.0000000000002524
Efficacy of acupuncture for whiplash injury
Whiplash associated disorder (WAD), caused by sudden cervical spine hyperflexion and hyperextension during motor vehicle accidents, is commonly associated with ongoing symptoms. This systematic review aimed to summarise and appraise the quality of the evidence for the use of acupuncture in the treatment of WAD.
Eleven databases were searched for published studies with no language restrictions from inception to 1st October 2023. Eligible studies were randomised controlled trials (RCTs) that used acupuncture to treat patients with WAD, including electroacupuncture and dry needling, either alone or combined with other treatments. WAD was classified using the Quebec Task Force diagnostic criteria. The comparator was usual care which could involve sham or conventional treatments other than acupuncture (e.g. physiotherapy, medication). The primary outcome was neck pain, measured using a visual analogue or numerical rating scale score. Secondary outcomes were cervical spine range of motion (ROM), the Neck Diasability Index (NDI) and adverse events. Study selection and assessment of methodological quality, using the Cochrane Collaboration Risk of Bias tool (version 2), were performed by two authors. Evidence certainty was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system. Meta-analyses using random and fixed effects models assessed standardised mean differences (SMDs) and 95% confidence intervals (CIs). Subgroup analyses were performed according to the type of acupuncture used.
Eight trials (n = 525) were included in the systematic review and seven trials (n = 502) in the meta-analysis. Five trials compared acupuncture to usual care, medication or sham. Types of acupuncture interventions studied included general acupuncture (5 trials), electroacupuncture (2 trials), and motion-style acupuncture treatment (MSAT) (1 trial). Five trials involved at least six sessions, one trial had between 2-6 sessions and one trial has one session. Only 5 out of 8 trials reported on adverse events. Six trials were rated as being at low risk of bias. High risk of bias was noted in deviations from intended interventions (1 trial); missing outcome data (2 trials); and measurement of the outcome (1 trial).
Compared to usual care, any type of acupuncture improved pain (SMD = -0.57, 95% CI: -0.86 to -0.28, I2= 51%, n = 423, 6 trials, moderate certainty evidence) and cervical spine extension ROM (SMD = 0.47, 95% CI: 0.05 to 0.89, I2= 56%, n = 216, 3 trials, low certainty evidence); but no between-group differences were found for other cervical spine ROM or the NDI (SMD = -0.17, 95% CI: -0.51 to 0.17, I2= 69%, n = 472, 6 trials). All reported adverse events were graded as mild, except for one which was moderate. According to subgroup analyses, only general acupuncture (SMD = -0.50, 95% CI: -0.93 to -0.06, I2= 40%, n = 152, 3 trials) and MSAT (SMD = -0.85, 95% CI: -1.27 to -0.44, n = 97, 1 trial) were effective for improving pain.
Following WAD a small number of studies demonstrated that acupuncture, either used alone or in combination with other treatments, may improve pain and extension ROM compared to usual care involving conventional or sham treatments. Treatment effects varied according to the type of acupuncture used.
Lee SH, Park SY, Heo I, Hwang EH, Shin BC, Hwang MS. Efficacy of acupuncture for whiplash injury: a systematic review and meta-analysis. BMJ Open. 2024 Jan 17;14(1):e077700. doi: 10.1136/bmjopen-2023-077700

Prevention of low back and pelvic girdle pain during pregnancy
During pregnancy, women may experience low back pain (LBP), pelvic girdle pain (PGP) or a combination of both (lumbopelvic pain [LBPP]) which impacts on activities of daily living and their quality of life. Incidence rates are estimated at between 57-90% for LBP and 4-76% for PGP. For women who experience LBP or PGP during pregnancy, up to half will continue to have some pain complaints one year after childbirth.
This systematic review aimed to investigate the short-term and long-term effectiveness and acceptability of a prevention strategy compared to control, on episodes of LBP, PGP or LBPP in women during pregnancy.
Electronic databases were searched from their inception to January 2023. Randomised and quasi-randomised controlled trials enrolling pregnant women without LBP or PGP at the onset of the study were included. Trials needed to compare an experimental group receiving a prevention strategy aimed at preventing LBP, PGP or LBPP during pregnancy to a control group receiving no intervention, placebo, sham or waitlist control. Trials also needed to include at least one of the outcomes of interest, i.e. incidence of LBP, PGP, or LBPP, sick leave and acceptability in the short-term [<12 week] and long-term [> 12 weeks]. Acceptability was measured by the number of participants who withdrew due to any reason out of total number of participants randomly assigned to each group. Risk of bias in each included trial was assessed using the PEDro scale.
Meta-analysis was conducted using a random-effects model, with the reporting of relative risk (RR) and 95% confidence intervals (CI). Trials were grouped by specific prevention strategy, outcome and time points. The GRADE approach was used to rate the certainty of evidence, with the quality of evidence beginning at moderate certainty because it was not possible to assess occurrence of publication bias (small number of trials).
This review included six randomised controlled trials enrolling 2231 pregnant women aged 23-31 years and gestational ages 12-24 weeks. All were low-risk single-child pregnancies and most women were considered sedentary. Eligible trials evaluated two strategies, education combined with exercise and stand-alone exercise. All trials were at a low risk of bias (median PEDro score 7, range 6 to 8). All trials provided data on new events of LBP, PGP or LBPP.
Stand-alone exercise likely reduces the risk of LBP (RR 0.92, 95% CI 0.85–0.99; 2 trials, n=621, moderate certainty evidence), has uncertain effects on reducing the risk of PGP (RR 0.87, 95% CI 0.53–1.44, 1 trial, n=105, very low certainty evidence) and likely does not reduce the risk of LBPP (RR 0.92, 95% CI 0.68–1.25, 2 trials n=1156, moderate certainty evidence) in the long-term. Stand-alone exercise is likely acceptable among women with LBPP (RR 0.60, 95% CI 0.42–0.84, moderate certainty evidence) but uncertain among women with LBP (low certainty evidence).
Education combined with exercise likely does not reduce the risk of LBP or PGP in the short-term (LBP: RR 1.06, 95% CI 0.85–1.31; PGP: RR 1.19, 95% CI 0.71–1.98) or long term (LBP: RR 1.05, 95% CI 0.85–1.30; PGP: RR 1.02, 95% CI 0.80–1.29) (2 trials, n= 438; moderate certainty evidence). There was uncertainty regarding education combined with exercise on LBPP (very low certainty evidence) and no difference between intervention and control groups for acceptability in the short term (very low certainty evidence) and long term (moderate certainty evidence) (2 trials, n=454).
Current moderate quality evidence supports stand-alone exercise as an acceptable intervention for pregnant women with lumbopelvic pain and has a small protective effect regarding episodes of low back pain in the long-term. Further high-quality studies are still required to confirm effects on preventing low back pain, pelvic girdle pain and lumbopelvic pain in the short and long-term.
Santos FF, Lourenço BM, Souza MB, Maia, LB, Oliveira VC, Oliveira MX. Prevention of low back and pelvic girdle pain during pregnancy: a systematic review and meta-analysis of randomised controlled trials with GRADE recommendations. Physiotherapy 118 (2023) 1–11 https://doi.org/10.1016/j.physio.2022.09.004

Some types of exercise are more effective than others in people with chronic low back pain: a network meta-analysis
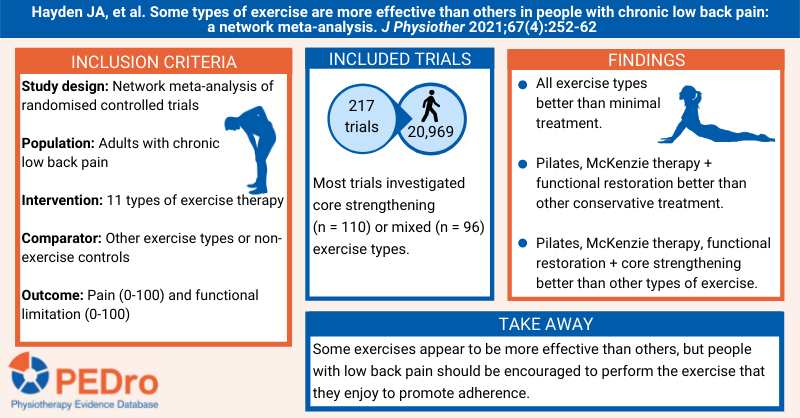
Guidelines recommend exercise as first line care for the treatment of chronic low back pain. A Cochrane review summarised in a PEDro blog in November 2021 concluded that exercise therapy most likely reduces pain when compared to minimal treatment, but the impact of exercise therapy on functional limitations when compared to minimal treatment and on pain and functional limitations when compared to other conservative care are probably small. However, this Cochrane review did not investigate the effects of different types of exercise therapy compared to non-exercise controls nor do any head-to-head comparisons of different exercise therapies. This network meta-analysis aimed to estimate the effects of different exercise therapies on pain and function compared to non-exercise controls and to other types of exercise in adults with chronic low back pain.
Guided by a prospectively registered protocol, sensitive searches were performed in seven databases (including Cochrane CENTRAL, Medline and PEDro) and two trial registries to identify randomised controlled trials evaluating exercise therapy for adults with low back pain (date of most recent search: 7 December 2020). The patients were adults with non-specific low back pain of at least 12 weeks duration. The intervention was any exercise therapy prescribed or planned by a health professional that involved conducting specific activities, postures and/or movements with a goal to improve low back pain outcomes. The type of exercise therapy was classified into 11 categories: general strengthening; stretching; core strengthening (or motor control); flexibility; aerobic; functional restoration; McKenzie therapy; Pilates; yoga; mixed; and, other. The comparators were non-exercise controls and a different category of exercise therapy. Non-exercise controls were classified as minimal treatment (no treatment, usual care, placebo, education, and ineffective interventions like electrotherapy) and other conservative treatment (psychological therapy, anti-inflammatory or analgesic medication, relaxation, manual therapy, physiotherapy not involving exercise, back school). The primary outcomes were pain intensity and functional limitations measured on any scale, and data were transformed to a 0-to-100-point scale (where 0 is no pain or functional limitation) for the analyses. A 15-point difference in pain and a 10-point difference in functional limitations were pre-specified to be clinically important. If outcomes were evaluated at multiple time points, data from the time point closest to 3 months post-randomisation were used in the primary analyses. Two independent reviewers selected trials for inclusion and evaluated trial quality, and disagreements were resolved by discussion or by arbitration from a third reviewer. Data were extracted by one reviewer and checked by at least one other reviewer. Trial quality was evaluated using the first version of the Cochrane risk of bias tool. The Confidence in Network Meta-Analysis (CINeMA) approach was used to evaluate certainty of evidence. Pair-wise meta-analyses and network meta-analysis was used to pool trials and calculate the mean between-group differences (and the associated 95% confidence intervals). The two non-exercise comparator categories (minimal treatment and other conservative treatment) and the 11 exercise categories were used as nodes in the network meta-analysis.
217 trials (20,969 participants) were included in the analyses. The average age of participants was 44 years, 56% were women and the average pain intensity at baseline was 51 on a 100-point scale. The 369 exercise groups were categorised as core strengthening (110 groups), mixed (96), general strengthening (44), aerobic (25), Pilates (24), stretching (17), other (15), yoga (13), functional restoration (10), McKenzie therapy (9), and flexibility (5). The 138 non-exercise comparison groups were categorised as minimal treatment (86 groups) and other conservative treatment (52).
All categories of exercise therapy reduced pain intensity (mean difference -19 to -7 points; low or moderate certainty) and functional limitations (-12 to -3; low to high) compared to minimal treatment. Pilates, McKenzie therapy, functional restoration, and core strengthening reduced pain (-11 to -6; low or moderate), and McKenzie therapy, flexibility, Pilates and functional restoration reduced functional limitation (-7 to -3; moderate) compared to other conservative treatment.
Some types of exercise were more effective than others.
- Pilates exercise reduced pain more than all other exercise categories (mean difference -12 to -4 points; low or moderate certainty) and reduced functional limitations more than stretching, other, aerobic, mixed, general strengthening, yoga, core strengthening and functional restoration (-7 to -3; moderate).
- McKenzie therapy reduced pain more than stretching, aerobic, flexibility, yoga, mixed, other and general strengthening (mean difference -8 to -4; moderate certainty), and reduced functional limitations more than stretching, other, aerobic, mixed, general strengthening, yoga, core strengthening and functional restoration (-8 to -4; moderate).
- Functional restoration exercise reduced pain more than stretching, flexibility, aerobic, yoga, mixed and other (mean difference -8 to -4; low or moderate certainty), and reduced functional limitations more than stretching, other, aerobic, mixed and general strengthening (-4 to -2; moderate).
- Core strengthening exercise reduced pain more than stretching, aerobic, flexibility, yoga and mixed (mean difference -6 to -5; low certainty), and moderate certainty evidence that core strengthening exercise reduced functional limitations more than stretching, other, aerobic and mixed (-3 to -2; low).
Pilates, McKenzie therapy, functional restoration and core strengthening exercise therapies were more effective than other types of exercise therapy for reducing pain intensity and functional limitations. Nevertheless, people with chronic low back pain should be encouraged to perform the exercise that they enjoy in order to promote adherence.
For readers who are not familiar with network meta-analysis, we recommend reading a research note on this topic published in the Journal of Physiotherapy .
Hayden JA, et al. Some types of exercise are more effective than others in people with chronic low back pain: a network meta-analysis. J Physiother 2021;67(4):252-62
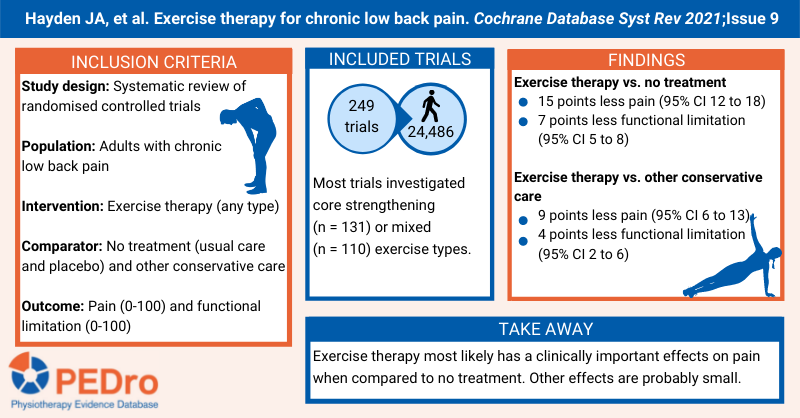
Exercise therapy for chronic low back pain
Low back pain is the leading cause of disability globally and results in enormous direct healthcare and lost productivity costs. Despite a large amount of research, there remains uncertainty about the best treatment approach for people with chronic non-specific low back pain. This systematic review aimed to estimate the effects of exercise therapy compared to control on pain and functional limitations in people with chronic non-specific low back pain.
Guided by a prospectively registered protocol, sensitive searches were performed in seven databases (including Cochrane CENTRAL, Medline and PEDro) and two trial registries to identify randomised controlled trials evaluating exercise therapy for people with low back pain (date of search: 27 April 2018). The population is adults with non-specific low back pain of more than 12 weeks’ duration. Trials that recruited participants with symptoms or signs consistent with radiculopathy (eg, leg pain) were included if back pain was their main complaint. Exercise therapy was classified as strengthening, stretching, core strengthening, flexibility/mobilising, aerobic, functional restoration, McKenzie therapy, yoga, mixed, and other. The comparator could be no treatment (including no or minimal treatment, usual care or placebo), other conservative treatments (including education, manual therapy, electrotherapy, psychological therapy, non-exercise physiotherapy, back school, relaxation, anti-inflammatory medication) or another type of exercise therapy. However, comparisons between different types of exercise therapy were not undertaken in this review. The primary outcomes were pain and functional limitations measured on any scale, and data were re-scaled to a 0-to-100-point scale (where 0 is no pain or functional limitations) for the analyses. A 15-point difference in pain and a 10-point difference in functional limitations were pre-specified to be clinically important. If outcomes were evaluated at multiple time points, data from the earliest time point after randomisation was used in the primary analyses. Two independent reviewers selected trials for inclusion and evaluated trial quality, and disagreements were resolved by discussion or by arbitration from a third reviewer. Data were extracted by one reviewer and checked by at least one other reviewer. Trial quality was evaluated using version 1.0 of the Cochrane risk of bias tool. The Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach was used to evaluate certainty of evidence. Meta-analysis was used to pool trials and calculate the mean between-group difference, and the associated 95% confidence interval (CI), for pain and functional limitations. Separate comparisons were performed for trials using no treatment and other conservative treatments as comparators.
249 trials (24,486 participants) were included in the review. Most trials were conducted in Europe (122 trials), Asia (38), North America (33) and the Middle East (24). The average age of participants was 44 years and 59% were women. At baseline, participants reported a mean pain intensity of 51 points and functional limitations of 38 points. 142 trials compared exercise therapy to no treatment or other conservative care. 151 trials compared the effects of two or more different types of exercise therapy. Most exercise therapy involved a mixed type of exercise (110 trial groups). The most common specific types of exercise therapy were core strengthening (131) and Pilates (29), general strengthening (57), stretching (51), and aerobic (41).
Compared to no treatment (including no or minimal treatment, usual care or placebo), exercise therapy reduced pain by a mean of 15 points (95% CI 18 lower to 12 lower; 35 trials; 2,746 participants; moderate certainty) and reduced functional limitations by a mean of 7 points (95% CI 8 lower to 5 lower; 38 trials; 2,942 participants; moderate certainty). This difference in pain was considered to be clinically important based on pre-specified criteria, but the difference in functional limitations was not.
Compared to other conservative care, exercise therapy reduced pain by a mean of 9 points (95% CI 13 lower to 6 lower; 64 trials; 6,295 participants; low certainty) and functional limitations by a mean of 4 points (95% CI 6 lower to 2 lower; 52 trials; 6,004 participants; moderate certainty). These differences were not considered to be clinically important.
Exercise therapy most likely reduces pain when compared to no treatment (including no or minimal treatment, usual care or placebo) in people with chronic non-specific low back pain. The impact of exercise therapy on functional limitations when compared to no treatment and on pain and functional limitations when compared to other conservative care are probably small.
Hayden JA, et al. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev 2021;Issue 9
Identification of subgroup effect with an individual participant data meta-analysis of randomised controlled trials of three different types of therapist-delivered care in low back pain
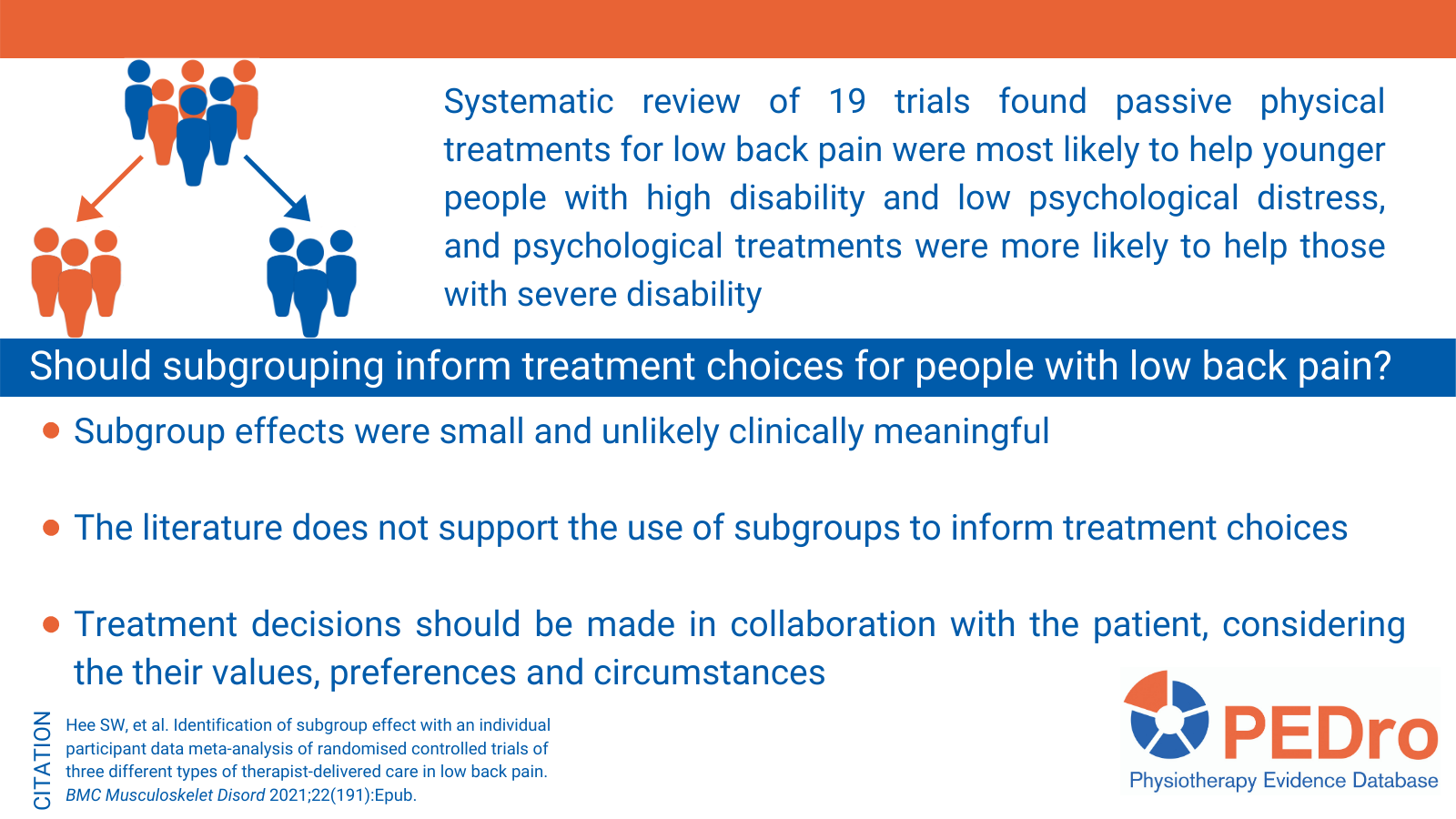
Proven treatments for low back pain only provide modest overall benefits. Matching people to treatments that are likely to be most effective for them may improve clinical outcomes and makes better use of healthcare resources. This systematic review aimed to understand which people with low back pain are most likely to benefit from different treatment approaches (active physical treatments, passive physical treatments, and psychological treatments).
Sensitive searches were performed in four databases, including Medline. Randomised controlled trials that had interventions delivered by a therapist and a sample size >179 were included. Since this was an individual patient data meta-analysis, authors of trials were invited to share data with the research team. Interventions were categorised as: control (non-active usual care), sham control (sham acupuncture, electrotherapy, advice/education, mock transcutaneous electrical nerve stimulation), active physical (exercise and graded activity), passive physical (individual physiotherapy, manual therapy, acupuncture) and psychological (advice/education, psychological therapy). Follow-up was classified as: short- (2 and 3 months), mid- (6 months) and long-term (12 months post randomisation). Thirty-two outcomes were classified into physical disability, pain, psychological distress and non-utility quality of life domains.
Pooled analyses were performed on individual patient data from at least two trials so as not to replicate original analyses. Missing data was not imputed. Potential moderators were identified from a previous systematic review on treatment moderators (ie, factors measured pre-randomisation indicating who benefits most and least from a treatment) and by including individual patient data from all trials in a single mixed-effects meta-analysis model for each follow-up time (with moderators declared statistically significant (p<0.05) or weakly significant (p<0.20)). Two approaches were used to identify sub-groups: Recursive Partitioning and Adaptive Refinement by Directed Peeling. Both aim to identify subgroups of participants who experience treatment effects larger than other participants.
19 trials (n=9,328 participants) were included in the analyses. The average age of participants was 49 years, 57% were female and the average Roland Morris Disability Questionnaire score at baseline was 10 out of 24 points (14 trials). Three treatment types were chosen for the exploration of potential moderators: active physical treatments, passive physical treatments, and psychological treatments. Control arms included non-active usual care and sham interventions. Age, gender, low back pain disability and severity, and psychological state were at least weakly significant in one or more of the moderator analyses and were considered for further subgroup analysis.
Participants with greater psychological distress and physical disability had the greatest improvement on the Mental Component Scale of Short Form Health Survey (12 or 36 item) from passive physical treatment compared to non-active usual care (treatment effects 4.3; 95% confidence interval (CI) 3.4 to 5.2). Recursive partitioning method found that participants with worse disability at baseline had the greatest reductions in disability measured using the Roland Morris Disability Questionnaire from psychological treatment compared to non-active usual care (treatment effects 1.7; 95% CI 1.1 to 2.3). Adaptive risk group refinement did not find any subgroup that would experience a larger benefit from psychological treatment over non-active usual care. Neither statistical method identified any subgroups that would experience a larger benefit from active physical treatment over non-active usual care.
Passive physical treatments for low back pain were most likely to help people who were younger with higher levels of disability and low levels of psychological distress. Psychological treatments were more likely to help those with severe disability. Active physical treatments appeared to help all subgroups equally. However, the size of the additional benefit achieved in the subgroups was small and unlikely to be clinically important. These findings do not support the use of sub-grouping for people with low back pain.
Hee SW, et al. Identification of subgroup effect with an individual participant data meta-analysis of randomised controlled trials of three different types of therapist-delivered care in low back pain. BMC Musculoskelet Disord 2021;22(191):Epub.
Prevention strategies to reduce future impact of low back pain
Low back pain is the leading cause of global disability and a common reason for absence from work, reduced productivity and seeking care. Prevention strategies are required to reduce the burden associated with this chronic, recurrent condition. This systematic review and meta-analysis aimed to estimate the effect of prevention strategies to reduce the impact of low back pain; as measured by pain intensity and associated disability.
Guided by a prospectively registered protocol, randomised controlled trials were identified through sensitive searches of five databases and citation tracking. Trials evaluating any strategy to reduce the future impact of low back pain, reporting pain intensity or disability at least 3 months after randomisation, and using a no intervention, placebo or minimal intervention control group were included. Prevention strategies could include any approach aiming to prevent or reduce the future impact of low back pain, including workplace interventions targeting risk factors or interventions to make people more fit, healthy or resilient. Trials evaluating the treatment of low back pain were excluded. The primary outcomes were pain intensity and disability (with data converted to a 0-100 point scale) in the short-term (6 months after randomisation) and long-term (12 months after randomisation). Risk of bias was assessed using the Physiotherapy Evidence Database scale and certainty of evidence was determined using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system. Trial selection, data extraction, and appraisal of risk of bias and certainty were independently performed by two reviewers, with any disagreements resolved through discussion. Meta-analyses were used to calculate mean between-group differences and 95% confidence intervals (CI) when trial interventions and populations were considered to be sufficiently similar.
Twenty-seven articles met the criteria to be included in the review. Of those, 21 trials (7,269 participants) published in 23 articles were included in the primary analyses. Prevention strategies were tested in three populations: working aged adults (18 trials, mainly recruited from hospitals or other workplaces, average age 45 years, 76% women), pregnant women (2 trials), and children (1 trial). Six different prevention strategies were evaluated in working aged adults: exercise (3 trials), exercise and education (5 trials), education (8 trials), ergonomics (3 trials), and ergonomics and education (2 trials) [note: some trials had multiple treatment arms so are included in more than one strategy]. Exercise was evaluated in pregnant women. Exercise combined with education was evaluated in children.
For working aged adults, exercise reduced future low back pain intensity (mean difference -5 points on a 100-point scale; 95% CI -7 to -2; 3 trials; 612 participants; moderate certainty) but not disability (-2; -7 to 2; 1 trial; 189 participants; very low certainty) in the short-term when compared to a control intervention. No trials evaluated the long-term outcomes associated with exercise. There was no effect of exercise and education on future low back pain intensity in the short-term (-2; -10 to 6; 3 trials; 184 participants; low certainty) or long-term (-4; -9 to 0; 4 trials; 471 participants; moderate certainty) or on disability in the short-term (-5; -13 to 3; 2 trials; 150 participants; low certainty) when compared to a control group. However, exercise and education did reduce disability in the long-term (-6; -10 to -3; 4 trials; 471 participants; moderate certainty). There was no effect of education alone on either future pain intensity in the short-term (-2; -5 to 1; 3 trials; 777 participants; moderate certainty) or long-term (2; -6 to 10; 2 trials; 126 participants; low certainty) or future disability in the short-term (-3; -6 to 1; 4 trials; 804 participants; moderate certainty) or long-term (0; -5 to 4; 2 trials; 176 participants; low certainty). There was no effect of ergonomics on future pain intensity in the short-term (1; -3 to 6; 1 trial; 552 participants; low certainty) or long-term (2; -3 to 7; 1 trial; 538 participants; low certainty) when compared to control interventions. No trials evaluated disability after ergonomic intervention. Similarly, there was no effect of ergonomics and education on future pain intensity in the short-term (1; 95% CI -7 to 9; 1 trial; 192 participants; very low certainty) or long-term (0; -7 to 7; 2 trials; 266 participants; low certainty) or on disability in the short-term (2; -2 to 6; 1 trial; 192 participants; very low certainty) or long-term (1; -3 to 6; 1 trial; 184 participants; very low certainty).
For pregnant women, exercise did not reduce future low back pain intensity (-3; -7 to 1; 2 trials; 452 participants; moderate certainty) or disability (-3; -7 to 1; 1 trial; 240 participants; low certainty) in the short-term, when compared to control interventions. No trials evaluated long-term outcomes.
For children, when compared to a control intervention, exercise and education did not reduce future low back pain intensity in the short-term (0; -12 to 12; 1 trial; 70 participants; very low certainty). No trials evaluated disability or long-term pain.
This review provides moderate quality evidence that an exercise program, or a program combining exercise and education, may reduce future low back pain intensity (short-term) and associated disability (long-term) in working aged adults. In contrast, interventions focusing on education and ergonomics (separately or in combination) are unlikely to reduce future low back pain intensity or disability in this patient group. Exercise probably doesn’t reduce future low back pain in pregnant women, and exercise and education may not reduce future low back pain in children.
de Campos TF, et al. Prevention strategies to reduce future impact of low back pain: a systematic review and meta-analysis. Brit J Sports Med 2020 Jul 9:Epub ahead of print

Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions
The aim of this systematic review was to evaluate the effectiveness of scoliosis-specific exercises compared with other non-surgical interventions for adolescent with idiopathic scoliosis. Studies were eligible if they were randomised controlled trials evaluating scoliosis-specific exercises in participants with idiopathic scoliosis (defined as a primary Cobb angle of at least 10 degrees) and aged between 10 years and skeletal maturity. Scoliosis-specific exercises were defined ‘specific movements performed with a therapeutic aim of reducing the deformity.’ Comparators were non-surgical interventions, including bracing, electrical stimulation, manual therapy, generalised exercise, sports, active recreational activities, advice or waiting list. Primary outcomes were Cobb angle (in degrees) and angle of trunk rotation.
The review identified 9 studies (480 participants) that were conducted in Egypt, Brazil, Italy, Turkey, Korea, China, and Canada. There was variability in terms of the exercise parameters prescribed across studies. Treatment duration ranged from 3 weeks to 42 months.
Compared to general exercise or standard care, there was very low quality evidence that scoliosis-specific exercises reduced the thoracic Cobb angle (3 studies, 125 participants, mean difference -7 degrees,95% confidence interval (CI) -9 to -5), lumbar Cobb angle (2 studies, 105 participants, mean difference -7 degrees, 95% CI -10 to -4), and main curve location (3 studies, 172 participants, mean difference -5 degrees, 95% CI -9 to -1). Compared to general exercises or standard care, there was very low quality evidence that scoliosis-specific exercises did not reduce the angle of trunk rotation (1 study, 25 participants, mean difference -1 degrees,95% CI -3 to 5).
Very low quality evidence supports the use of scoliosis-specific exercise rather than standard care or other types of exercise for patients with adolescent idiopathic scoliosis to reduce spinal curvature. Large-scale and rigorous randomised controlled trials are required to evaluate the effectiveness and cost-effectiveness of scoliosis-specific exercise.
Thompson JY, et al. Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions: a systematic review and meta-analysis. Physiotherapy 2019;105(2):214-34
Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain
This systematic review evaluated the benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain. Randomised controlled trials conducted in adults 18 years and older with more than 50% of participants reporting pain lasting more than 3 months were included. Spinal manipulative therapy was compared against guideline-recommended interventions, non-guideline-recommended interventions, sham spinal manipulation, and combined therapies. Risk of bias was assessed using the criteria described by Cochrane Back and Neck Review group. Primary outcomes were pain intensity (0-100 scale) and back specific functional status. Treatment effects were reported at 1, 3, 6 and 12 months post-randomisation.
47 trials were included (n = 9,211 participants). Several health professionals were involved in providing treatment, with most being chiropractors (16 studies) or physiotherapists (14 studies).
Compared to guideline-recommended interventions, moderate quality evidence suggests that spinal manipulative therapy was not better for pain at 1 month (mean difference -3.17, 95% confidence interval (CI) -7.85 to 1.51) and 12 months (mean difference -1.86, 95% CI -4.79 to 1.07). A statistically significant difference was found at 6 months (mean difference -3.09, 95% CI -5.42 to -0.77) but this was not considered to be clinically relevant. Compared to interventions not recommended by guidelines, spinal manipulative therapy was significantly better at reducing pain at 1 month (mean difference -7.48, 95% CI -11.50 to -3.47, high quality evidence), 6 months (mean difference -7.54, 95% CI -13.29 to -1.79, moderate quality evidence), and 12 months (mean difference -7.80, 95% CI-14.19 to -1.41). Compared to sham spinal manipulation, there was low quality evidence that spinal manipulative therapy did not reduce pain at 1 month (mean difference -7.55, 95% CI -19.86 to 4.76), and very low quality evidence that it did not reduce pain at 6 months (mean difference 0.96, 95% CI -6.34 to 8.26) and 12 months (mean difference 0.20, 95% CI -5.33 to 5.37).
For back specific functional status, there was moderate quality evidence that spinal manipulative therapy was statistically better to guideline-recommended treatments at 1 month, but not at 6 and 12 months. Compared to interventions not recommended by guidelines, there was high quality evidence that spinal manipulative therapy was significantly better at 1 month, and these effects were clinically relevant, with moderate and low quality evidence that spinal manipulative therapy was statistically and clinically better than interventions not recommended by guidelines at 6 and 12 months, respectively. Compared to sham spinal manipulation, there was low quality evidence that spinal manipulation improved functional status at 1 month, and this improvement was clinically relevant.
Spinal manipulative therapy produces similar effects to guideline-recommended therapies for chronic low back pain, and it appears to be better than non-guideline-recommended interventions for improvement in function in the short-term.
Rubinstein SM, et al. Benefits and harms of spinal manipulative therapy for the treatment of chronic low back pain: systematic review and meta-analysis of randomised controlled trials. BMJ 2019;364:l689
Effectiveness of telephone-based interventions for managing osteoarthritis and spinal pain
This systematic review assessed whether real-time telehealth interventions reduce pain intensity and disability in people with osteoarthritis of the knee and hip or spinal (back or neck) pain compared to usual care or face-to-face interventions. Types of telehealth interventions included interventions delivered remotely by any person (i.e., therapist, health professional or trained operator) by telephone or videoconferencing in which there was a direct person-to-person verbal exchange of information. The primary outcomes were pain intensity and disability. Risk of bias was assessed with the Cochrane risk of bias tool. The quality of the evidence was evaluated using the GRADE approach. In total, 15 randomised controlled trials were included in the meta-analyses (n=2789 participants). Meta-analysis of data from five studies (n=1357 participants) revealed moderate quality evidence of a small intervention effect of telephone-based interventions with educational materials on pain intensity when compared to usual care (standardised mean difference -0.27, 95% CI -0.53 to -0.01). Positive effects were found for spinal pain (standardised mean difference -0.55, 95% CI -0.92 to -0.19) but not for osteoarthritis. Meta-analysis of seven studies (n=1537 participants) revealed moderate quality evidence of a small effect of telephone-based interventions with educational materials on disability when compared to usual care (standardised mean difference -0.21, 95% CI -0.40 to -0.02). Again, positive effects were found for spinal pain (standardised mean difference -0.64, 95% CI -1.01 to -0.27), but not for osteoarthritis. There was moderate quality evidence that telephone intervention plus face-to-face intervention did not improve pain or disability compared to usual care or face-to-face intervention alone. Telephone-based services offer the potential to support people with spinal or osteoarthritis pain to access better quality care.
O’Brien KM et al. Effectiveness of telephone-based interventions for managing osteoarthritis and spinal pain: a systematic review and meta-analysis. PeerJ 2018;6:e5846
Upper limb
Shoulder stabilization versus immobilization for first-time anterior shoulder dislocation: a systematic review and meta-analysis of level 1 randomized controlled trials
Anterior shoulder dislocations are among the most common shoulder injuries in adolescent athletes and often occur after acute trauma. Despite multiple studies comparing rates of recurrent instability after surgical stabilisation and non-operative sling immobilisation for patients experiencing a first-time anterior shoulder dislocation, there remains uncertainty about the best treatment approach.
This systematic review aimed to estimate the effects of surgical stabilisation for people with a first-time anterior shoulder dislocation on recurrent instability, need for a future stabilisation procedure, range of motion, and function compared to sling immobilisation.
Searches were performed in seven databases (including PubMed, Embase, and Cochrane Library) to identify randomised controlled trials investigating the effects of surgical stabilisation versus sling immobilisation for the treatment of first-time anterior shoulder dislocation on rates of recurrent instability.
The outcomes were recurrent instability, subsequent stabilisation surgery, range of motion, function as assessed by the Western Ontario Shoulder Instability Index, and complications. Only outcomes reported by at least three trials were included. Two independent reviewers selected trials for inclusion. Disagreements were resolved by discussion or by arbitration from a third reviewer. Data were extracted by one reviewer and checked by a second. Trial quality was evaluated using version 1.0 of the Cochrane risk of bias tool. Meta-analysis was used to pool trials and calculate the between-group risk ratio, and the associated 95% confidence interval (CI), for recurrent instability and subsequent stabilisation surgery.
Five trials (259 participants) were included in the review. The average age of participants and percentage of males was 24 years and 87% in the operative group, and 23 years and 89% in the non-operative group. Four trials used similar arthroscopic Bankart procedures, and one used an open Bankart procedure. Participants in all trials underwent surgery between 10 and 28 days after anterior shoulder dislocation and were placed in an internally rotated sling immobiliser for 1-4 weeks post-operatively. The non-operative approach in 4 trials involved placing participants in an internal rotation sling for 1-4 weeks. In 1 trial, participants were placed in an external rotation and abduction immobiliser for 3 weeks. Physiotherapy protocols were identical between the operative and non-operative groups across trials and involved minimal active or passive movement through the immobilisation phase (about 3 weeks), active external rotation and abduction until 6 weeks, unrestricted range of motion after 6-12 weeks, and resistance exercises thereafter. All trials were at high risk of bias due to being unable to blind participants (performance bias) and therapists and/or outcome assessors (detection bias).
Surgical stabilisation reduced the risk of recurrent instability by 83% (95% CI 67% to 92%) and the risk of subsequent stabilisation surgery by 83% (95% CI 59% to 93%) compared to sling immobilisation. Findings were the same when only including trials in which participants in the non-operative group were immobilised in internal rotation. All 3 trials that assessed range of motion found no difference between surgical stabilisation and sling immobilisation. Of the 3 trials that assessed Western Ontario Shoulder Instability Index scores, 1 found higher scores in the operative group and 2 found no difference. Two complications were reported in the operative group and none in the non-operative group.
Surgical stabilisation for a first-time anterior shoulder dislocation reduces the risk of recurrent instability and need for a future stabilisation procedure compared to non-operative management involving sling immobilisation. It is uncertain whether surgical stabilisation is superior to non-operative management for improving shoulder function and range of motion.
Belk JW, et al. Shoulder stabilization versus immobilization for first-time anterior shoulder dislocation: a systematic review and meta-analysis of level 1 randomized controlled trials. Am J Sports Med 2022 Feb 11:Epub ahead of print.
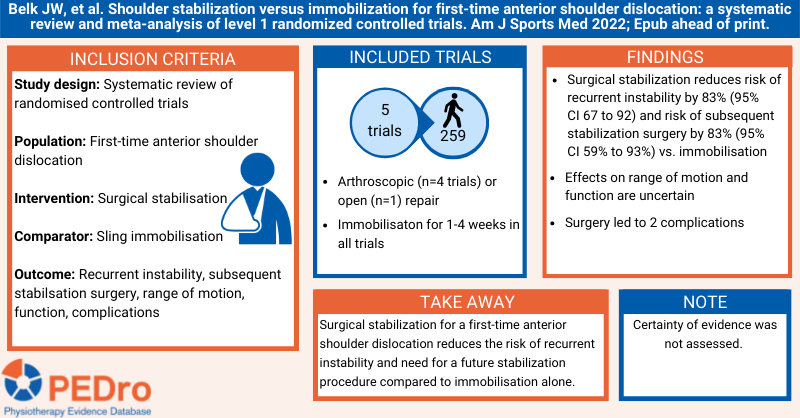
Effectiveness of progressive and resisted and non-progressive or non-resisted exercise in rotator cuff related shoulder pain
Shoulder pain is a common musculoskeletal complaint, of which rotator cuff related pain is the predominant diagnosis. Clinical guidelines recommend exercise for rotator cuff related pain but make no distinction about the type of exercise prescribed. This review aimed to estimate the average effect of resisted and progressive exercise and non-resisted or non-progressive exercise, both compared to no treatment or placebo.
Sensitive searches were performed in five databases (Cochrane CENTRAL, Medline, Embase, CINAHL, OpenGray) and two clinical trial registries (ClinicalTrials.gov, who.int/ictrp). Randomised controlled trials of exercise compared to no treatment or placebo in participants over 16 years of age with a primary complaint of rotator cuff related pain of any duration were included. Exercise was classified as resisted and progressive (ie, explicitly stated how resistance was applied and that there was progression of the volume or the load, or both, over time) or non-resisted or non-progressive (ie, explicitly stated that load was not applied or not progressed, or both). The primary outcome was a composite measure of pain and function measured on any shoulder-specific scale (converted to a 0-100 scale, with 0 being no pain or dysfunction). Secondary outcomes were pain (overall, with activity, and pain at rest; all converted to a 0-100 scale, with 0 being no pain) and the number of participants experiencing an adverse event. Medium-term (6 weeks to 6 months) follow-up was used as the primary timepoint. Two reviewers independently identified trials for inclusion and extracted data, with discrepancies resolved through discussion or by arbitration from a third reviewer. The Cochrane risk of bias tool was used to evaluate trial quality, with all quality ratings extracted from a recent Cochrane review (Page et al, 2016). Confidence in the evidence was conducted using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Random effects meta-analysis was used to calculate the mean difference and 95% confidence interval (CI) for the composite measure of pain and function and the pain-related secondary outcomes, and the relative risk and 95% CI for adverse events.
Seven trials (468 participants) were included in the analyses: 4 trials (271 participants) evaluated resisted and progressive exercise and 3 trials (197 participants) evaluated non-resisted or non-progressive exercise. The mean age of participants was between 47 and 61 years old and trials largely included males. Baseline composite pain and function was comparable (33 to 50 out of 100).
Compared to no treatment or placebo, resisted and progressive exercise reduces composite pain and dysfunction by a mean of 15 points (95% CI 9 to 21, 4 trials, 271 participants), overall pain by 11 points (95% CI 6 to 16, 3 trials, 197 participants), pain with activity by 25 points (95% CI 14 to 36, 2 trials, 135 participants), and pain at rest by 23 points (95% CI 14 to 32, 2 trials, 135 participants). All results were classified as low certainty. The effect on adverse events is unclear as no trials reported whether any adverse events occurred.
No effect was observed for non-resisted or non-progressive exercise. Compared to no treatment or placebo, non-resisted or non-progressive exercise reduced composite pain and dysfunction by a mean of 4 points (95% CI -2 to 9, 3 trials, 197 participants), overall pain by 3 points (95% CI -1 to 8, 3 trials, 197 participants), pain with activity by 3 points (95% CI -5 to 12, 3 trials, 197 participants), and pain at rest by 2 points (95% CI -7 to 10, 2 trials, 174 participants). Adverse events (short term increase in pain) may be higher with non-resisted or non-progressive exercise compared with placebo (risk ratio 3.77, 95% CI 1.49 to 9.54, 1 trial, 116 participants). Again, all results were classified as low certainty.
Resisted and progressive exercise provides an uncertain clinically meaningful improvement in pain and function compared to no treatment or placebo among people with rotator cuff related pain. In contrast, there is low certainty evidence of no benefit in all outcomes with non-resisted or non-progressive exercise.
Naunton J, et al. Effectiveness of progressive and resisted and non-progressive or non-resisted exercise in rotator cuff related shoulder pain: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil 2020 Jun 22:Epub ahead of print.
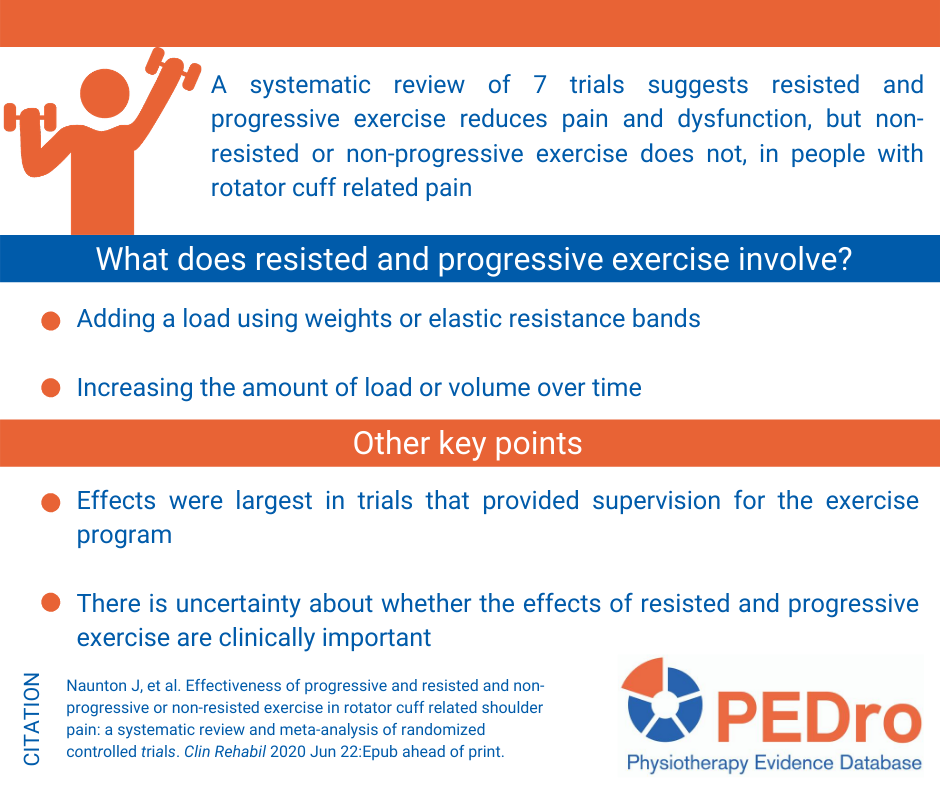
Lower limb
Interventions for improving mobility after hip fracture surgery in adults
Improving mobility outcomes after hip fracture is key to recovery. Mobility is the ability to move about, including standing up and walking and mobility strategies are treatments that aim to help people move better. This Cochrane systematic review aimed to evaluate the benefits and harms of interventions for improving mobility and physical functioning after hip fracture surgery in adults.
This Cochrane systematic review included randomised controlled trials or quasi-randomised controlled trials that assessed mobility strategies after hip fracture surgery. Eligible trials were identified from 8 electronic databases. Trials were included if they investigated the effect of strategies aimed to improve mobility. These could include care programmes, exercise (gait, balance, functional training, strength/resistance/endurance/flexibility training, three-dimensional exercise and general physical activity) or muscle stimulation. Interventions could be compared to usual care (both in-hospital), no intervention, sham exercise or social visits (post-hospital). Critical outcomes were mobility, walking speed, functioning, health-related quality of life, mortality, adverse effects, and return to living at pre-fracture residence.
Two reviewers identified and selected studies, extracted data, and assessed risk of bias using the Cochrane Risk of Bias 2.0 tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
The review included 40 randomised controlled trials (n = 4059 participants) from 17 countries. Patients were mostly elderly (average age 80 years) and female (80%). All trials had unclear or high risk of bias for one or more domains.
In the hospital setting, there is low certainty evidence that mobility strategies may lead to a moderate, clinically meaningful increase in mobility compared to usual care (standardised mean difference [SMD]: 0.53, 95% confidence interval [CI] 0.10 to 0.96; n = 360). Post-hospital, there is high certainty evidence that mobility strategies compared to usual care, no intervention, sham exercise or social visit led to a small, clinically meaningful increase in mobility (SMD: 0.32, 95% CI 0.11 to 0.54; n= 761). Adverse events were rarely measured by included trials so the safety of these programs in the hospital and out of hospital settings remains unknown.
Compared with conventional care, interventions that target improvement in mobility after hip fracture may improve mobility and walking speed, both in hospital and post-hospital settings. However, long term and economic outcomes have not yet been determined.
Fairhall NJ, Dyer SM, Mak JC, Diong J, Kwok WS, Sherrington C. Interventions for improving mobility after hip fracture surgery in adults. Cochrane Database Syst Rev. 2022 Sep 7;9(9):CD001704.
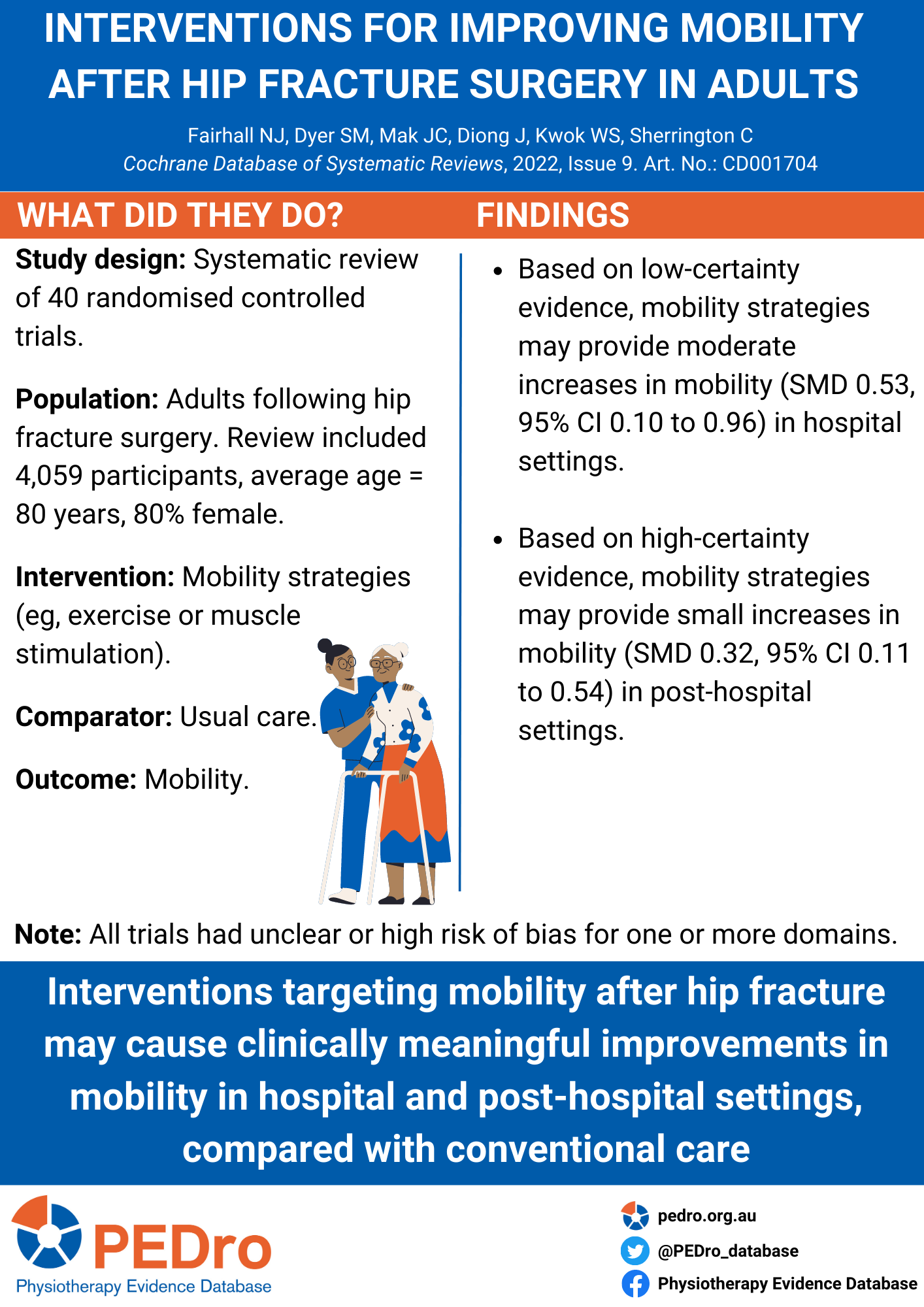
The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery: a systematic review and meta-analysis of randomised controlled trials
Ankle fractures are common injuries that often require open reduction and internal fixation surgery. Post-operative rehabilitation protocols traditionally recommend late weight-bearing to avoid complications. Recently, early weight-bearing has been explored as an alternative approach to potentially accelerate recovery. This systematic review aimed to examine the effects of early weight-bearing compared to late weight-bearing on function, time to return to daily life, and safety outcomes following ankle fracture surgery.
Seven electronic databases were searched for randomized controlled trials published in English and Chinese. Eligible studies included people recovering from ankle fracture surgery of any age, with no significant co-morbidities (e.g., severe cardiovascular disease, unstable chronic conditions, or acute neurological impairments). The intervention was defined as early weight-bearing protocols, encompassing both partial and complete weight bearing, initiated within six weeks post-surgery. The comparator was late weight-bearing, starting six weeks or more post-surgery. Primary outcomes were 1) ankle function, 2) time to return to daily life and 3) complication rates. (e.g., re-fracture, wound infection). A primary timepoint post-surgery was not specified. Risk of bias was assessed using the Cochrane Risk of Bias 1.0 tool. Meta-analyses were applied using fixed effects model (if I2 < 50%) or random-effects model (if I2 > 50%). There was no assessment of the certainty of evidence.
There review included 11 trials (862 participants). Eight (73%) trials initiated early weight-bearing within six weeks post-surgery. Some trials presented an unclear or high risk of bias due to lack of concealed allocation (5 trials), blinding of participants or personnel (7 trials), and blinding of outcome assessors (4 trials).
Compared to late weight-bearing, early weight-bearing improved ankle function scores at 6 weeks (SMD 0.69, 95% CI 0.49 to 0.88, I2 = 0%), 12 weeks (SMD 0.57, 95% CI 0.22 to 0.92, I2 = 75%), 24-26 weeks post-surgery (SMD 0.52, 95% CI 0.20 to 0.85, I2 = 51%), although ankle function was not improved 1-year post-surgery (SMD 0.21, 95% CI -0.01 to 0.42). Time to return to daily life was significantly shorter in patients who received early weight-bearing (MD -2.74 weeks, 95% CI -3.46 to -2.02, I2 = 0%). Early weight-bearing did not significantly increase complications compared to late weight-bearing (RR 1.30, 95% CI: 0.85 to 1.98).
Early weight-bearing after ankle fracture surgery improves ankle function more than late weight bearing in the short term but not at 1-year post-surgery. People who receive early weight-bearing have less time away from daily life without an increase in complication rates. These findings suggest that early weight-bearing could be used instead of late weight bearing post-operative ankle fracture.
Chen B, Ye Z, Wu J, Wang G, Yu T. The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery: a systematic review and meta-analysis of randomised controlled trials. Journal of Foot and Ankle Research Published online Jun 17 2024. doi/10.1002/jfa2.12011

Do exercise-based prevention programmes reduce non-contact musculoskeletal injuries in football (soccer)?
Football (soccer) is a popular sport world-wide. Despite the health benefits of playing football, non-contact musculoskeletal injuries (eg, hamstring strain) are relatively common. Exercise-based programs have been developed to prevent injury, but previous evaluations have not differentiated between contact and non-contact injuries. This systematic review aimed to estimate the effects of exercise-based programs compared to control to prevent non-contact musculoskeletal injuries in football players.
Guided by a prospectively registered protocol, sensitive searches of six databases (including Medline, Embase and PEDro), three clinical trial registries and citation tracking were performed to identify randomised controlled trials evaluating exercise-based injury prevention programs. The participants were football players aged 13 years and older. The intervention was any exercise therapy performed to develop function, skills or physical fitness. The comparator could be usual training or warmup, minimal intervention, education or no intervention. The primary outcome was the occurrence of any acute sudden onset musculoskeletal injury that occurred without physical contact with another player or object on the field. In addition to reporting the number of non-contact injuries, included trials needed to report the number of exposure hours for each group. Two reviewers independently selected trials and extracted data. Disagreements were resolved through discussion or arbitration by a third reviewer. Risk of bias was evaluated using the PEDro scale, with scores downloaded from the PEDro database and confirmed by one reviewer. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The number of non-contact injuries and exposure hours were used to calculate the injury incidence rate per 1,000 hours and the injury risk ratio. Meta-analysis was used to compute the pooled injury risk ratio and its 95% confidence interval (CI). One pre-planned subgroup analysis was undertaken based on exercise type: focused/unimodal (exercises chosen to train and protect a specific muscle or joint) vs. generalised/multimodal (exercises that targeted many body segments) on non-contact hamstring injuries.
10 trials (13,355 participants) were included in the meta-analyses. The trials were conducted in the United States, Norway, and the Netherlands (2 trials each) and in Germany, Japan, Nigeria and Sweden (1 trial each). Only male players were included in 6 trials and only female players in 4. Most trials (7) recruited youth players and all trials included amateur players. The duration of the exercise-based program ranged from 3 to 9 months. Focused exercise was used in 3 trials (Nordic Hamstring Exercise, Bounding Exercise Program) and generalised exercise in 7 (Prevent Injury and Enhance Performance Program, FIFA 11+, FIFA 11, Knäkontroll (neuromuscular training)). All interventions were applied at least twice a week to every training session.
Exercise-based programs reduce the risk of non-contact injuries by 23% compared to control, with an injury risk ratio of 0.77 (95% CI 0.61 to 0.97; 10 trials; 13,355 participants; low certainty). The sub-group analysis revealed that focused programs were not different from generalised programs for the prevention of non-contact hamstring injuries. The injury risk ratio was 0.65 (0.44 to 0.97; 3 trials; 1,238 participants; low certainty) for focused programs and 0.63 (0.19 to 2.12; 3 trials; 2,573 participants; very low certainty) for generalised programs.
Exercise-based prevention programs may reduce the risk of non-contact musculoskeletal injuries in football players. Hamstring-focused programs did not reduce hamstring injury any more than general programs.
Lemes IR, et al. Do exercise-based prevention programmes reduce non-contact musculoskeletal injuries in football (soccer)? A systematic review and meta-analysis with 13,355 athletes and more than 1 million exposure hours. Br J Sports Med 2021 May 17:Epub ahead of print
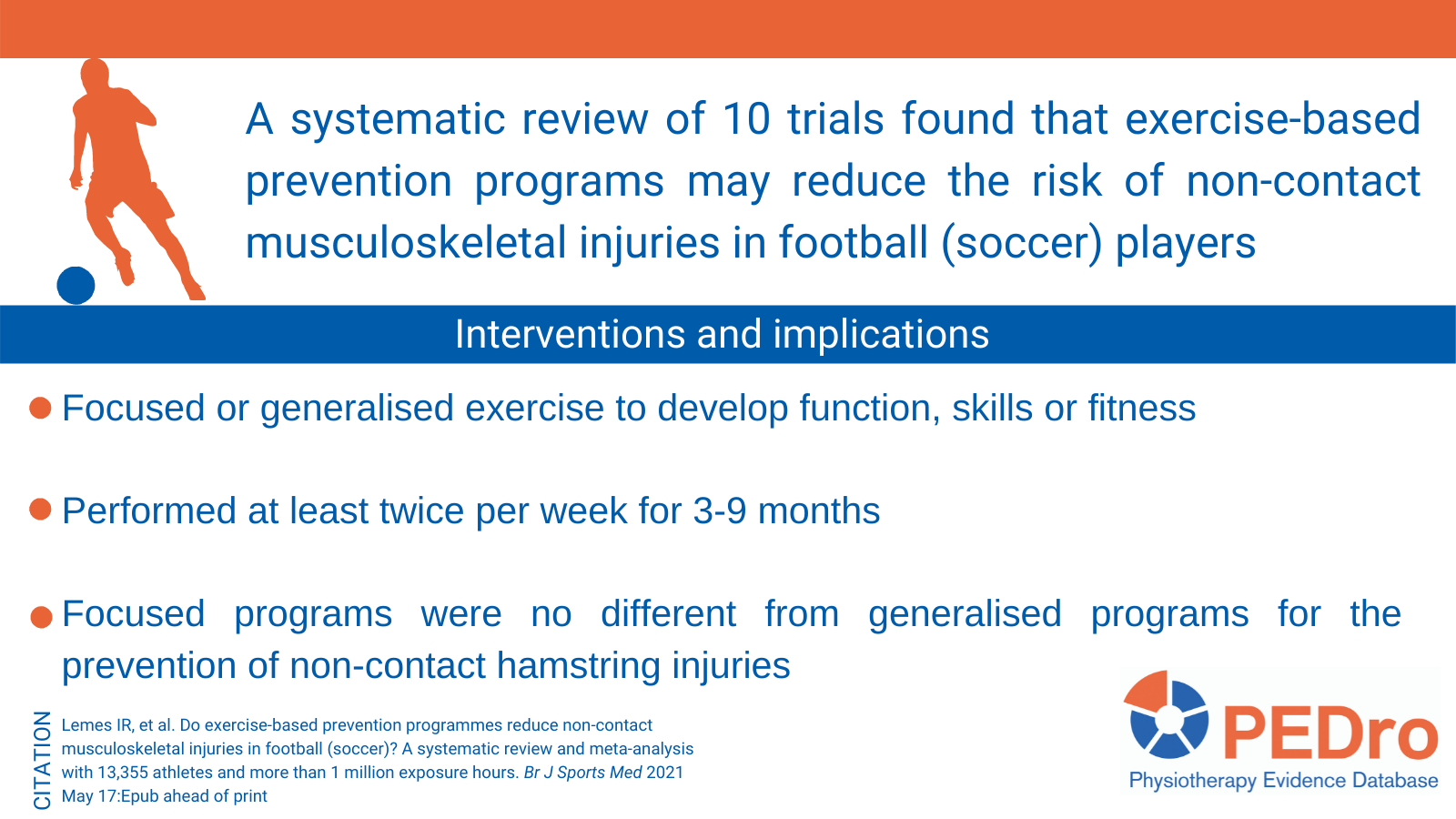
Tai Chi exercise can ameliorate physical and mental health of patients with knee osteoarthritis
Knee osteoarthritis is a common and disabling condition. Previous reviews of Tai Chi for knee osteoarthritis have focused on physical health outcomes. This systematic review aimed to estimate the effects of Tai Chi compared to non-exercise intervention (eg, education), usual care or physiotherapy on both physical and mental health in people with knee osteoarthritis.
Searches were performed in eight databases (including PubMed, Embase and PEDro). Randomised controlled trials that involved participants with knee osteoarthritis and compared Tai Chi to non-exercise intervention (eg, education), usual care or physiotherapy were included. Key outcomes were physical and mental health. Two reviewers independently selected trials for inclusion, extracted data, and evaluated trial quality and certainty of evidence. Disagreements were resolved by discussion or arbitration from a third reviewer. Trial quality was evaluated using the Cochrane risk of bias tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Meta-analyses were used to calculate the standardised mean between-group difference (and its 95% confidence interval (CI)) of change from baseline to follow-up for each outcome.
16 trials (986 participants) were included in the meta-analyses. The trials were conducted in the United States (n=7 trials), China (6) and Korea (3) and recruited people with knee osteoarthritis with a mean age of 60 to 79 years. About 80% of participants were women. Three styles of Tai Chi were evaluated (Yang (n=7 trials), Sun (3), Qigong (1), unclear (5)), and treatment duration ranged from 8 to 52 weeks. Tai Chi was compared to usual care in 9 trials, education in 5 trials, and physiotherapy in 2 trials. Physical health was quantified using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) physical function subscale in 13 trials (note: lower scores indicate better function, so a negative between-group difference indicates better physical function in the Tai Chi groups). Mental health was quantified using the 36-Item Short Form Survey (SF-36) mental component summary score in 5 trials (note: higher scores indicate better mental health, so a positive between-group difference indicates better mental health in the Tai Chi groups).
Mean physical health in the Tai Chi groups was 0.9 standard deviations lower than in the control groups (95% CI 0.7 to 1.1 lower; 13 trials; 844 participants; moderate certainty). This translates to an absolute mean lowering of 8 points (95% CI 6 to 10 lower) on the 0- to 68-point WOMAC physical function subscale compared to control (note: the baseline standard deviation from the Osteoarthritis Initiative study and guidance from the Cochrane Handbook v6.1 were used to calculate this estimate).
Mean mental health in the Tai Chi groups was 0.3 standard deviations higher than in the control groups (95% CI 0.1 to 0.5 higher; 5 trials; 409 participants; moderate certainty). This translates to an absolute mean difference of 2 points (95% CI 1 to 4) on the 0- to 100-point SF-36 mental component summary score (note: the baseline standard deviation from Wang et al 2016 was used to calculate this estimate).
Tai Chi probably improves physical and mental health in people with knee osteoarthritis. The small difference in the SF-36 mental component summary score is unlikely to be clinically meaningful.
Hu L, et al. Tai Chi exercise can ameliorate physical and mental health of patients with knee osteoarthritis: systematic review and meta-analysis. Clin Rehabil 2020 Sep 21:Epub ahead of print
Treatment and prevention of acute and recurrent ankle sprain
This study is an overview of intervention systematic reviews. The authors included 46 systematic reviews evaluating treatment and preventive strategies for acute ankle sprain and chronic ankle instability. The reviews included provided data from 309 individual studies. The primary outcomes were injury or re-injury incidence and function. The secondary outcomes were pain, strength, range of motion, proprioception and muscle activity in the ankle joint, and performance measures (i.e., biomechanical analyses of static or dynamic postural control, gait or jumping or landing tasks). The quality of the reviews was assessed using the AMSTAR tool and had a mean score of 6.5 out of 11. There is consistent evidence for exercise therapy and external supports (e.g., bracing, taping) for preventing ankle re-injury incidence (odds ratio 0.59, 95% confidence internal (CI) 0.51 to 0.68; odds ratio 0.38, 95% CI 0.30 to 0.47, respectively). For the treatment of acute ankle sprain, there is consistent evidence for non-steroidal anti-inflammatory drugs, early mobilisation, and exercise therapy for improving pain, swelling and function. There is limited evidence supporting the use of manual therapy for treating acute ankle sprain, although it does improve dorsiflexion range of motion. The efficacy of surgery and acupuncture are controversial and there is insufficient evidence to recommend ultrasound in the treatment of acute ankle sprains. There is a lack of evidence for orthotics or footwear for chronic ankle instability. The limitations of this review include the data extraction being conducted by only one reviewer and the high heterogeneity in the data presented in the included reviews.
Doherty C et al. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med 2017;51(2):113-25
Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players
In this new systematic review, the authors included 5 studies (4 cluster randomised controlled trials and 1 cohort study) that investigated injury prevention programs that included the Nordic Hamstring exercise on the hamstring injury rate in soccer players. Pooled data of 4,455 individuals included in the 5 studies were analysed. A total of 315,992 exposure hours and 166 hamstring injuries were collected from the included studies. The pooled results showed 51% overall injury reduction per 1,000 hours of exposure for to injury prevention programs that included the Nordic hamstring exercise compared to controls (injury risk ratio = 0.49; 95% confidence interval = 0.291 to 0.827; p = 0.008). A limitation of this review is that it was not possible to evaluate the isolated effect of Nordic Hamstring exercise because the injury prevention programs included a variety of other exercises. Another limitation is that cost effectiveness was not considered as an outcome in the review, even though economic data have been published.
Al Attar WS, et al. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: a systematic review and meta-analysis. Sports Med 2017;47(5):907-16.