Return to all evidence summaries
Neurology
Neurology includes, but is not restricted to, lesions of the central and peripheral nervous systems excluding those whose primary presentation is pain or paraesthesia such as carpal tunnel syndrome, neuralgia or sciatica.
The most recently synthesised review is at the top of the list.
- Aquatic Compared With Land-Based Exercises on Gross Motor Function of Children/Adolescents With Cerebral Palsy
- Backward walking training is as effective as or better than forward walking training for improving walking speed after stroke
- Effects of rehabilitation exercise program types on dynamic balance in patients with stroke
- Changes in walking speed following resistance training in people with multiple sclerosis
- Effects of exercise on depressive symptoms in patients with Parkinson Disease
- Home-based is as effective as centre-based rehabilitation for improving upper limb motor recovery and activity limitations after stroke
- Physical exercise for people with Parkinson’s disease
- Neuromuscular electrical stimulation improves activities of daily living post stroke
- Electromechanical-assisted training for walking after stroke
- Organised inpatient (stroke unit) care for stroke
- Aerobic exercise interventions reduce blood pressure in patients after stroke or transient ischaemic attack
- Supervised lifestyle intervention for people with metabolic syndrome improves outcomes and reduces individual risk factors of metabolic syndrome
- Exercise therapy for functional capacity in chronic diseases
- Exercise to prevent falls in older adults
- Interventions involving repetitive practice improve strength after stroke
- Mirror therapy for improving motor function after stroke
- Circuit class therapy for improving mobility after stroke
- Repetitive task training for improving functional ability after stroke
Aquatic Compared With Land-Based Exercises on Gross Motor Function of Children/Adolescents With Cerebral Palsy
Cerebral palsy (CP) is a common childhood disability characterised by motor impairments that affect mobility and functional skills. Rehabilitation programs aim to improve fitness, mobility, and participation through interventions such as fitness, strength and mobility training and task-specific exercises. Aquatic-based exercises, which utilise water’s buoyancy and thermal effects, may reduce joint stress, promote trunk control and muscle activation and enhance motivation. Previous systematic reviews have evaluated aquatic therapy benefits but have not compared aquatic- and land-based exercise effects on gross motor function in this population. The aim of this systematic review and meta-analysis was to compare the effects of aquatic-based versus land-based exercises on gross motor function in children and adolescents with CP.
The review followed PRISMA guidelines and was prospectively registered on PROSPERO (CRD42020194121). Searches across eight databases (PubMed, Cochrane Library, Scopus, Web of Science, EMBASE, SciELO Citation Index, LILACS and CINAHL), citation tracking and clinical trial registries of randomised controlled trials (RCTs) involving children aged 2–18 years with CP. Eligible interventions were structured aquatic-based exercises compared with land-based programs. Outcomes were measured using standardised tools such as the Gross Motor Function Measure (GMFM). Data extraction was performed independently by three reviewers. Risk of bias was assessed using the PEDro scale, and evidence quality was rated using GRADE. Meta-analyses were conducted using fixed-effects models. Effect sizes were reported standardized mean differences (SMD) with 95% confidence intervals. Subgroup analyses evaluated the effects of different aquatic exercise types (aquatic physical therapy, Halliwick method, swimming exercises, gait training and water exercises).
Fifteen RCTs published between 2007 and 2023 were included, involving 369 participants aged 2–18 years. Most participants were ambulatory and classified as Gross Motor Function Classification System levels I–III with spastic hemiparetic or diparetic CP. Interventions varied: five studies used aquatic physical therapy, five applied the Halliwick method, three focused on swimming, one on gait training in water, and one on aqua-plyometric exercises. Land-based programs included neurodevelopmental treatment approaches, functional activities and combinations of stretching, strengthening, gait and balance training. Most interventions lasted 10–12 weeks, with session durations 30–60 minutes, twice weekly. Risk of bias was high overall, frequently due to lack of concealed allocation, incomplete follow-up and lack of intention-to-treat analysis; only six studies were rated as good quality.
Meta-analysis of 13 trials (n=253) showed very low-quality evidence that aquatic-based exercises improved gross motor function compared to land-based exercises (SMD 0.45, 95% CI 0.24 to 0.66, p<0.001), indicating a small effect size. Subgroup analysis revealed low quality evidence of benefit for aquatic physical therapy (SMD 0.47, 95% CI 0.05 to 0.89, 4 trials, n=93, p=0.03). No significant differences for Halliwick method (SMD 0.33, 95% CI -0.01 to0.67, 4 trials, n=138, p=0.06, low quality evidence) or swimming exercises (SMD 0.47, 95% CI -0.09 to 1.03, 3 trials, n=52, p=0.10). Overall, heterogeneity was low (I²=0 to 5%), but methodological limitations and small sample sizes reduced confidence in findings. Few studies reported on adverse events and they were not assessed in the review.
Aquatic-based exercises, particularly aquatic physical therapy, may offer small improvements in gross motor function compared to land-based programs for children and adolescents with CP. However, evidence quality was low due to high risk of bias, small sample sizes, and intervention heterogeneity. Aquatic therapy could serve as an adjunct or alternative to land-based therapy, but decisions should consider accessibility, cost, and patient preference. Future research should involve well-designed trials with adequate sample sizes and standardised protocols.
Pauluka E, Ceolin LS, Fontanela LC, Dos Santos AN. Aquatic Compared With Land-Based Exercises on Gross Motor Function of Children/Adolescents With Cerebral Palsy: A Systematic Review With Meta-Analysis. Child Care Health Dev. 2025 Jan;51(1):e70023. doi: 10.1111/cch.70023.

Backward walking training is as effective as or better than forward walking training for improving walking speed after stroke
Recovery of walking in people following stroke is often the main goal for patients, which is primarily achieved with forward walking training. It is hypothesised that the use of backward walking training may better improve the kinematic parameters of walking compared to forward walking; however, no review has explored the effect of backward walking compared to forward walking. This systematic review aimed to estimate the effects of backward walking training compared to forward walking training on walking in people after stroke.
Eight databases including PEDro, EMBASE, Medline, Scielo, AMED, Cochrane Central Register of Systematic Reviews, Cochrane Central Register of Controlled Trials, and LILACS were searched for randomised controlled trials (RCTs). Reference lists of relevant articles were also searched. No date or language restrictions were applied to the search. RCTs were eligible if participants were adults following acute stroke (≤6 months) or chronic stroke (>6 months); intervention included backward walking training, either alone or in combination with forward walking training; and the comparator was forward walking training only. Outcome measures included walking speed (metres/sec), cadence (steps/min), and stride length (metres), which is typically calculated using a timed walk test e.g., 10 m walk test, or a 3D movement analysis system. Titles and abstracts were screened for eligibility by one reviewer. Two reviewers independently screened full texts for eligibility, with disagreements resolved by a third reviewer. Data extraction of included studies was completed by two reviewers, with details of unavailable information sought from corresponding authors. Two reviewers independently evaluated the risk of bias using the PEDro scale. The overall evidence quality and strength of recommendations for outcomes was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system. A random effects meta-analysis was conducted.
Ten studies involving 247 participants were included. The mean age of participants ranged from 50 to 68 years, and the mean time since stroke ranged from 1 month to 7 years. The mean baseline walking speed ranged from 0.2 to 1.0 m/s. Studies investigated the effect of backward walking training only (n = 3) or backward walking combined with forward walking training delivered overground or on treadmills (n = 7). Training progression was achieved by increasing speed, distance, or modifying manual assistance and bodyweight support with increasing speed or distance. Training sessions lasted 20-70 mins, 3-6 times per week for 3-8 weeks.
Meta-analysis demonstrated that backward walking training compared to forward walking training improved walking speed (MD = 0.16 m/s, 95% CI 0.06 to 0.27, n = 156, 6 trials, I2 = 0%, moderate quality evidence), but showed no effect on cadence (MD = 3 steps/min, 95% CI −2 to 6, n = 156, 6 trials, I2 = 0%) or stride length (MD 0.03 m, 95% CI −0.02 to 0.09, n = 156, 6 trials, I2 = 0%). When compared to forward walking only, backward walking training combined with forward walking training improved walking speed (MD = 0.03 m/s, 95% CI 0.01 to 0.04, n = 91, 4 trials, I2 = 7%, low quality evidence), cadence (MD = 5 steps/min, 95% CI 1 to 10, I2 = 4%, n = 75, 3 trials, low quality evidence), and stride length (MD = 0.04 meters, 95% CI −0.01 to 0.09, I2 = 5%, n = 75, 3 trials, low quality evidence). Beyond the intervention period, there was no effect of backward walking compared to forward walking on walking speed (MD = 0.06, 95% CI -0.11 to 0.22, n = 54, 2 trials, I2 = 0%, low quality evidence), cadence (MD = 3, 95% CI -2 to 8, n = 54, 2 trials, I2 = 0%, low quality evidence), and stride length (MD = 0.04, 95% CI -0.01 to 0.16, n = 54, 2 trials, I2 = 0%, low quality). The mean PEDro score of the included studies was 6 (range 4-8). The number of adverse events was not reported.
Moderate quality evidence supports backward walking training as being as or more effective for improving walking speed than forward walking training only; however, the maintenance of this effect beyond the intervention period remains uncertain.
Menezes KK, Avelino PR, Ada L, Nascimento LR. Backward walking training is as effective as or better than forward walking training for improving walking speed after stroke: a systematic review with meta-analysis. Top Stroke Rehabil. 2025;32(5):531-543. doi:10.1080/10749357.2024.2420547
Effects of rehabilitation exercise program types on dynamic balance in patients with stroke
This systematic review aimed to evaluate the effects of rehabilitation exercise programs on dynamic balance in people more than 6 months post-stroke.
Recovery of balance and postural control after stroke is a major predictor of disability as it directly affects the patient’s achievement of independent daily living and quality of life. Common methods used in clinical settings to improve balance and postural control in stroke patients include strength training, isokinetic trunk training, trunk stabilization training, and task-oriented approaches. Dynamic balance training has been used to regain balance control however the effect of the type of exercise intervention applied to stroke patients’ balance and posture control is not yet clear. In particular, factors such as duration of intervention, type, and individual characteristics of patients lead to variation in effectiveness.
Three databases were searched (Medline, Web of Science, and ProQuest) for randomised controlled trials (RCTs) published between January 2018 and October 2022. Eligible studies included patients with a stroke onset greater than 6 months ago, intervention was exercise programs such as virtual reality, aquatic activities, dual-task exercise, balance training, physical activity, gait exercise, resistance exercise, and trunk control exercise on dynamic balance in stroke patients. Studies using robots, stimulation therapy and passive treatments were excluded. The outcome measure was limited to the Berg Balance Scale. The comparators were experimental and controlled groups.
The study selection process was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) process with two researchers who searched, screened, and compared literature through keywords. Data analysis calculated the effect size (<0.2 small, 0.2-0.79 medium, ≥0.8 large). Publication bias was tested using a Forest Plot, Trim and Fill, and the quality of each study was evaluated through the diagnostic test of Comprehensive Meta-Analysis program ver.3 (CMA3) program.
Thirty trials with 540 participants were included. The mean age was 59.8 years old and stroke onset period was 27.1 months. Heterogeneity was assessed through the Cochrane’s Q and inconsistency test (I2), and a random effect model was used.
The overall effect of exercise for balance and postural control in stroke patients was medium (0.550 , 95% CI 0.331 to 0.769), according to the Cohen’s standard. No publication bias was detected, and the quality of the analysed papers was assessed as good.
Subgroup analyses were performed based on the level of heterogeneity for gender, age, period of onset, and types of exercise was calculated. Gender had a moderate effect size in males (0.551) and females (0.458). Exercise programs for balance were found to have the highest effect on stroke patients aged 60-64) when the time of stroke onset was greater than 50 months (1.060). However, the 95% CI for subgroup analyses and adverse events were not reported.
The subgroup analysis on exercise program type showed large effect sizes in balance training (0.966; 95% CI 0.552 to 1.380; 5 studies) and aquatic activities (0.830; 95% CI -0.251 to 1.912; 3 studies), moderate effect sizes in virtual reality (0.762; 95% CI 0.116 to 1.409; 3 studies), physical activity (0.581; 95% CI -0.657 to 1.819; 3 studies), gait training (0.541; 95% CI 0.130 to 0.951; 6 studies), dual-task (0.478; 95% CI 0.152 to 0.804; 3 studies), trunk control (0.284; 95% CI -0.092 to 0.659; 4 studies), and small effect sizes in resistance training (0.128; 95% CI -0.785 to 0.529; 3 studies). Balance training, dual-task, gait training, and virtual reality variables differed statistically significantly.
Exercise programs are effective in improving dynamic balance in stroke patients, with balance training having the highest effect size, particularly for when the time from onset of stroke is longer.
Han B, Lee J, Yim S, Kim D. Effects of rehabilitation exercise program types on dynamic balance in patients with stroke: a meta-analysis of randomized controlled trials. Topics in Stroke Rehabilitation 2024;31(7):681-691.
Changes in walking speed following resistance training in people with multiple sclerosis
Systematic review found that resistance training improves walking speed among people with multiple sclerosis.
Individuals with multiple sclerosis (MS) often have muscular weakness, fatigue, ataxia and balance impairments. This can often negatively contribute to their walking ability, especially walking speed. This systematic review aimed to investigate the effects of lower limb resistance training on walking speed in individuals with MS.
Seven databases were searched for randomised controlled trials (RCTs) published in English. The databases included CINAHL, Medline, The Allied and Complimentary Medicine Database, Web of Science, Physiotherapy Evidence Database (PEDro), PsycINFO, and Sports Medicine and Education Index. Full text articles were screened by two reviewers and disagreements resolved by a third reviewer. Eligible studies included people aged ≥ 18 years with a diagnosis of MS (disease duration, phenotype of MS and disability level was disregarded), resistance training interventions for the lower limbs (with or without supervision, regardless of duration of intervention or training session frequency, duration, intensity, volume) and outcomes included 1 or more objective measure of walking speed. Resistance training was any type of exercise using a variable amount of external resistance completed over one or more sets of a certain number of repetitions. Excluded studies were interventions that combined resistance training with other interventions, outcomes of overall functional mobility (e.g., timed up and go test). The comparator was active control (hatha yoga, mobility exercise, home based neurofunctional training, balance and motor control training, circuit endurance training) or no-intervention control. The outcome was walking speed, measured by standardised walking test measures. The methodological quality of included studies was assessed using the PEDro scale for RCTs, independently evaluated by two reviewers. and any disagreements resolved by a third reviewer.
Twelve studies, involving 425 participants were included . The Expanded Disability Status Scale was used to assess disability, ranging from 1.0 to 6.0, indicating mild to moderate disability. Of those studies who reported MS phenotypes, 322 had relapsing-remitting MS, 35 had secondary progressive MS, and 22 had primary progressive MS. Six studies recruited relapsing-remitting MS participants only. Of all participants, 180 participants received resistance training, 139 participants received no interventions and 85 participants received an active control. Across all studies, five outcome measures were used: 10-Meter Walk Test (10MWT), Timed 25-Foot Walk Test (T25FWT), 50-Meter Walk Test (50MWT), 2-Minute Walk Test (2MWT), 6-Minute Walk Test (6MWT). Seven articles included lower body exercises, four articles included upper and lower body exercises of which two studies also included core exercises. One study compared a high intensity concentric resistance training program of the less affected/stronger ankle dorsiflexor muscles to one training the more affected/weaker ankle dorsiflexor muscles. The methodological quality of the trials ranged from 3 to 8 on the PEDro scale.
Of the 12 studies, eight studies found a within-group improvement for the effect of resistance training on at least one measure of walking speed. Six studies compared the effects of resistance training with no-intervention controls but only one study found a significant between-group difference between post intervention favouring the resistance training group. No studies found significant between changes favouring the resistance training group when compared with the active control group. Seven studies that compared the effects of resistance training with no-intervention controls were included in a meta-analysis. When results were pooled within a random effects model, a significant improvement in walking speed of 0.10m/s (95% CI 0.01 to 0.19) was found favouring the intervention (p < 0.05 with high heterogeneity (I2 = 83%). As a result, a sensitivity analysis involving results from short walking tests (10MWT, T25FWT, 50MWT) showed a larger overall effect on walking speed (0.13 m/s, 95% CI 0.04 to 0.23, p < 0.05). Comparatively, results from longer walking tests (2MWT, 6MWT) showed a smaller improvement in walking speed (0.09 m/s, 95% CI 0.01 to 0.17, p < 0.05).
Resistance training improves walking speed compared to active control and no-intervention controls among people with MS.
McManaman, C., Novak, B., Paul, L., & Rooney, S. Changes in walking speed following resistance training in people with multiple sclerosis: A systematic review and meta-analysis. PM&R. 2025 Feb;17(2):222-37.
Effects of exercise on depressive symptoms in patients with Parkinson Disease
Parkinson’s Disease is a neurodegenerative disorder, which results in both motor and non-motor impairments. Depression is one of the most common non-motor symptoms for people with Parkinson’s Disease, ranging from 20-50%, with a 2022 systematic review and meta-analysis finding an overall prevalence of 38%. Depression in Parkinson’s Disease has been associated with worse motor symptoms, disability and quality of life. Exercise has been shown to result in smaller increases in Leva-dopa medications, improvements in gait speed and endurance, less disability and improved quality of life, but it’s effect on depressive symptoms is unclear. This systematic review aimed to estimate the effects of physical exercise interventions compared to control on depressive symptoms in people with Parkinson’s Disease, and also to investigate whether the effects differ by exercise type or intensity.
A search of two databases (PubMed and Web of Science) from inception to February 2022 was performed to identify randomised controlled trials evaluating physical exercise interventions. The participants were people with Parkinson’s Disease (no age range specified). The intervention was any type of physical exercise training of more than one session. The comparator could be either mild and regular physical activity programs (e.g. stretching only) or no physical exercise training. The primary outcome was the change in depressive symptoms. Three reviewers independently selected the trials, extracted data and evaluated trial quality. Disagreements were resolved through arbitration by a fourth reviewer. Trial quality was assessed using the Cochrane risk of bias tool, however no tool was used to evaluate the certainty of the evidence. Individual effect sizes were quantified for each study by calculating standardised mean differences (SMD) and 95% confidence intervals (CI). Then overall effect sizes were estimated by statistically incorporating individual effect sizes, using a random-effects meta-analysis model. Pre-defined moderator variable analyses were performed to determine whether the effects differ by exercise type (e.g. aerobic, strength, balance, flexibility or combined training) or intensity (e.g. light-moderate or moderate-vigorous).
Nineteen trials (1,302 participants) published between 2015 and 2021 were included in this review. Some trials had more than one exercise intervention and there were 23 total comparisons from the 19 trials. The trials were conducted in 10 countries from Asia, Europe, North and South America. All trials included men and women, with a range of mean age at enrolment of 59.3 to 75.5 years and range of mean disease duration of 1.8 to 8.0 years. Frequency of training was 1 to 5 sessions per week and the duration of the exercise programs ranged from 3 to 288 weeks, with most from 13 to 26 weeks. Combined exercise programs (e.g. balance and strength) were the most common type (14 programs), followed by aerobic training only (five programs), then flexibility training only (two programs) and one program each for strength training only and balance training only. Of the 14 combined training programs, 12 included aerobic training. Moderate-vigorous intensity exercise programs were the most common (17 programs) and six exercise programs involved light-moderate intensity exercise.
Overall, physical exercise interventions had significant positive effects on the reduction in depressive symptoms in patients with Parkinson’s Disease with a SMD of 0.83 (95%CI 0.52 to 1.14). The pre-defined moderator variable analysis revealed that combined exercise training programs had significant positive effects on the reduction in depressive symptoms in patients with Parkinson’s Disease with a SMD of 1.11 (95%CI 0.64 to 1.59), however neither aerobic training alone nor flexibility training alone had a significant effect. The other pre-defined moderator variable analysis revealed that both exercise intensities had significant positive effects on the reduction in depressive symptoms in patients with Parkinson’s Disease (light-moderate exercise intensity SMD of 0.97 (95%CI 0.52 to 1.42) and moderate-vigorous exercise intensity SMD of 0.78 (95%CI 0.41 to 1.15)).
Physical exercise interventions have significant and large positive effects on the reduction in depressive symptoms in patients with Parkinson’s Disease. These effects are more closely associated with exercise type than exercise intensity.
Kim R, Lee TL, Lee H, Ko DK, Jeon B, Kang N. Effects of exercise on depressive symptoms in patients with Parkinson Disease. Neurology 2023; 100:e3777-e387.
Home-based is as effective as centre-based rehabilitation for improving upper limb motor recovery and activity limitations after stroke
This systematic review aimed to estimate the effects of home-based exercises compared to centre-based exercises on improving motor dexterity, recovery, strength, upper-limb movement performance, upper-limb movement quality and participation in people with acute to chronic stroke.
This review included randomised controlled trials that investigated the effectiveness of home-based exercise compared to centre-based exercises for adults at any time after stroke. Eligible trials were identified from seven electronic databases. Trials were included if they compared home-based exercise (at least 2/3 of the exercise was performed at home) targeting the paretic upper-limb with a minimum of 4 sessions over a minimum of 2 weeks and control group of centre-based exercises provided in a hospital, private practice or community centre. Impairments and activity were measured by six outcomes of interest: dexterity (e.g., 9-hole peg test), motor recovery (e.g., The Box and Block Test), strength (e.g., dynamometry), upper-limb movement performance (e.g., Box and Block test), upper-limb movement quality (e.g., Motor Activity Log), and participation (e.g., Assessment of Life Habits). No outcome was nominated as primary.
The review included 8 randomised controlled trials. There were 488 participants aged 55 to 70 years in the acute/sub-acute phase (1 trial), chronic phase (2 trials) and both acute and chronic phase (5 trials). Exercises were completely supervised, semi-supervised in person, or remotely supervised. For home-based exercises, participants trained for 40-120 minutes per session, 5 times per week for 4-13 weeks. The control groups had similar dosages and were performed mainly in clinics.
For impairments, there was no difference between home-based exercise centre-based exercise for upper-limb movement performance for dexterity (MD -0.01 pegs/s, 95% CI -0.04 to 0.05; 5 trials, 212 participants, moderate certainty evidence), motor recovery (MD 1.4 points, 95% CI -0.9 to 3.8; 5 trials, 212 participants, moderate certainty evidence), and strength (MD 0.30 kg, 95% CI -2.4 to 3.0; 1 study, 88 participants, low certainty evidence).
For activity limitations, there was no difference between home-based exercise centre-based exercise for upper-limb movement performance (SMD -0.04, 95% CI -0.25 to 0.18; 4 studies, 328 participants, high certainty evidence) and upper-limb movement quality (MD 0.11 points 95% CI -0.23 to 0.44; 3 studies, 198 participants, moderate certainty evidence).
No studies assessed the effect of home-based exercise and centre based exercise on participation.
Home-based exercise is similar to centre-based exercise in people with stroke for improving dexterity, motor function, strength, upper-limb movement performance and upper-limb movement quality following stroke. This indicates that the location that exercises take place is less important than the amount and type of exercise. This may have implications for people with limited access to healthcare facilities such as those living in rural or remote locations.
Nascimento LR, Gaviorno LF, Brunelli M, Gonçalves JV, da Silva Arêas FZ. Home-based is as effective as centre-based rehabilitation for improving upper limb motor recovery and activity limitations after stroke: A systematic review with meta-analysis. Clinical Rehabilitation 2022, 36(12): 1565–1577. DOI: 10.1177/02692155221121015

Physical exercise for people with Parkinson’s disease
This Cochrane systematic review aimed to estimate the effects of different types of physical exercise compared to another type of exercise, control group or both on the severity of motor signs, quality of life and occurrence of adverse events in people with Parkinson’s Disease (PD).
This Cochrane systematic review included randomised controlled trials that assessed physical exercise interventions for people with PD. Eligible trials were identified from eight electronic databases. Trials were included if they compared one type of physical exercise to another type of exercise, a control, or both. Critical outcomes were; severity of motor signs, reported using the motor scale from the Unified Parkinson Disease Rating Scale (UPDRS-M); quality of life, reported using the Parkinson’s Disease Questionnaire 39 (PDQ-39); and occurrence of adverse events, which was measured by the number of participants with any adverse advent. Two reviewers independently identified and selected studies, extracted data, and assessed risk of bias using the Cochrane Risk of Bias 2.0 tool. Confidence in the evidence was evaluated using the CINeMA approach.
The review included 156 randomised controlled trials (7,939 participants) from over 20 countries. Participants had mostly mild to moderate disease, no major cognitive impairment and a mean/median age range between 60 to 74 years. For the outcome severity of motor signs (71 studies; 3196 participants), there is high confidence that dance has a moderate beneficial effect (mean difference (MD) -10.32, 95% confidence interval (CI) -15.54 to -4.96) and low confidence that aqua-based, gait/balance/functional, and multi-domain training might have a moderate beneficial effect (aqua-based: MD -7.77, 95% CI -13.27 to -2.28; gait/balance/functional: MD -7.37, 95% CI -11.39 to -3.35; multi-domain: MD -6.97, 95% CI -10.32 to -3.62). There is low confidence that flexibility training might have a trivial or no effect (MD: 2.01, 95% CI -4.82 to 8.98), and very low confidence and high uncertainty about the effects of strength/resistance training (MD: -6.97, 95% CI -11.93 to -2.01).
For the outcome quality of life (55 studies; 3283 participants), there is moderate confidence that aqua-based training probably has a large beneficial effect (MD -14.98, 95% CI -23.26 to -6.52), low confidence that endurance training might have a moderate beneficial effect (MD -9.16, 95% CI -15.68 to -2.82), and that gait/balance/functional and multi-domain training might have a small beneficial effect (gait/balance/functional: MD -5.64, 95% CI -10.04 to -1.23; multi-domain: MD -5.29, 95% CI -9.34 to -1.06). There is very low confidence and high uncertainty about the effects of strength/resistance training and flexibility training (strength/resistance MD: -6.34; 95% CI -12.33 to -0.35; flexibility MD: 1.23, 95% CI -11.45 to 13.92).
There is very uncertain evidence about the effect of physical exercise on increasing the occurrence of adverse events.
Most physical exercise interventions provide beneficial effects on the severity of motor signs and quality of life for people with PD managing mild to moderate disease, with little evidence of differences between interventions. Although evidence for the effect of exercise on the occurrence of adverse events is very uncertain, the interventions included in the review were considered to be relatively safe.
Ernst M, Folkerts A-K, Gollan R, Lieker E, Caro-Valenzuela J, Adams A, Cryns N, Monsef I, Dresen A, Roheger M, Eggers C, Skoetz N, Kalbe E. Physical exercise for people with Parkinson’s disease: a systematic review and network meta-analysis. Cochrane Database of Systematic Reviews 2023, Issue 1. Art. No.: CD013856. DOI: 10.1002/14651858.CD013856.pub2.

Neuromuscular electrical stimulation improves activities of daily living post stroke
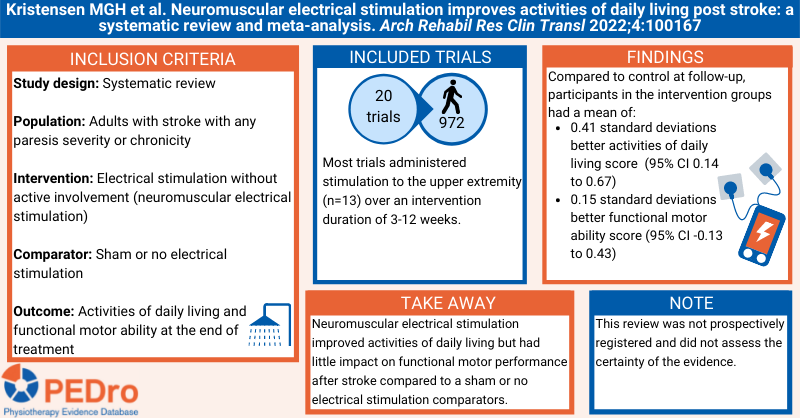
Stroke is a leading cause of disability and is typically associated with loss of motor function and reduced ability to perform activities of daily living. Electrical stimulation is recommended in clinical guidelines, but previous systematic reviews have not differentiated between different levels of patient involvement during the application of stimulation. This review aimed to estimate the effect of electrical stimulation without active involvement (neuromuscular electrical stimulation) compared to no electrical stimulation on activities of daily living and functional motor ability in adults with stroke.
A protocol that was specified a priori guided the methods. Sensitive searches performed in five databases (including PubMed and PEDro) and citation tracking were used to identify randomised controlled trials that were published in English. Participants were adults with clinically diagnosed stroke with any level of paresis severity or chronicity. Intervention was neuromuscular electrical stimulation administered to either the upper or lower limb through surface electrodes to elicit a visible muscle contraction with no active involvement from the patient plus usual rehabilitation. The comparator was usual rehabilitation only. The primary outcome was activities of daily living. Functional motor ability was the secondary outcome. Two independent reviewers selected trials for inclusion, evaluated risk of bias and extracted data. Any disagreements were resolved by consensus discussions or by a third reviewer. Risk of bias was evaluated using the PEDro scale and the Cochrane risk of bias tool. Certainty of evidence was not evaluated. Meta-analysis was used to pool the included trials to calculate standardised mean differences and 95% confidence intervals (CI). Three subgroup analyses were specified: location of stimulation (upper vs. lower limb); time post-stroke (acute vs. subacute vs. chronic); and, severity of paresis (mild vs. moderate vs. severe).
20 trials (956 participants) were included in the meta-analyses. Participants had a mean age of 62 years and were predominantly male (54%). The location of stimulation was the upper limb in 13 trials (primarily shoulder abductors, wrist extensors) and the lower limb in 7 trials (primarily ankle dorsiflexors). The time post stroke was acute (ie, < 7 days) for 3 trials, subacute (ie, 7 days to 6 months) for 13 trials and chronic (ie, > 6 months) for 4 trials. The severity of paresis was moderate in 5 trials and severe in 6 trials, with no trials investigating participants with mild paresis, 5 trials having a range of severities and 4 trials not reporting severity. The intervention was applied for 10-60 minutes/session, 1-4 sessions/day and 3-7 days/week for 3-12 weeks. Cyclic stimulation was typically used (frequency 30 Hz, fixed pulse width of 200-300 microseconds) with the amplitude adjusted to achieve a visible muscle contraction or joint movement. 13 trials scored 6/10 or more on the PEDro scale.
Compared to control, participants in the neuromuscular electrical stimulation groups had a mean of 0.41 standard deviations better activities of daily living score (95% CI 0.14 to 0.67; 10 trials; 428 participants) at follow-up. This translates to a mean of 9 points more on the 0-100 version of the Barthel Index (95% CI 3 to 15), the scale most used to measure activities of daily living in the review, for neuromuscular electrical stimulation compared to control. [Note: the baseline standard deviation for the Barthel Index from an inception cohort study and guidance from the Cochrane Handbook v6.1 were used to calculate this estimate]. Compared to control, the mean functional motor ability score was 0.15 standard deviations higher in the electrical stimulation groups (95% CI -0.13 to 0.43; 13 trials; 659 participants). Because the 95% CI for this estimate includes zero, the intervention may have no effect for this secondary outcome.
Subgroup analyses revealed that effects for activities of daily living were slightly larger for the upper limb (standardised mean difference 0.34, 95% CI 0.04 to 0.64; 6 trials; 266 participants) than for the lower limb (standardised mean difference 0.49, 95% CI -0.04 to 1.03; 4 trials; 162 participants). Effects were also slightly larger in subacute stroke (standardised mean difference 0.44, 95% CI 0.10 to 0.78; 7 trials; 310 participants) than in chronic stroke (standardised mean difference 0.35, 95% CI -0.14 to 0.84; 3 trials; 118 participants), and there were no trials for this outcome for acute stroke. Severe paresis (standardised mean difference 0.36, 95% CI -0.55 to 1.26; 3 trials; 142 participants) and moderate paresis (standardised mean difference 0.21, 95% CI -0.16 to 0.58; 3 trials; 119) had similar effects, with no data being available for mild paresis.
Neuromuscular electrical stimulation provided in addition to usual rehabilitation improved activities of daily living post stroke more than usual rehabilitation alone. This was particularly evident for the upper limb and in subacute stroke. Neuromuscular electrical stimulation had little impact on functional motor ability.
Kristensen MGH et al. Neuromuscular electrical stimulation improves activities of daily living post stroke: a systematic review and meta-analysis. Arch Rehabil Res Clin Transl 2022;4:100167
Electromechanical-assisted training for walking after stroke
Improving walking is one of the main goals of rehabilitation after stroke. Electromechanical or robotic devices allow people with stroke with impaired walking to participate in intensive, high repetition, walking practice. This systematic review aimed to estimate the effects of electromechanical- or robot-assisted gait training and normal care compared to normal care alone on the ability to walk independently in people with stroke.
Guided by a protocol, sensitive searches were conducted in 11 databases (including Cochrane CENTRAL, Medline, Embase and PEDro) and two trial registers to identify randomised controlled trials in adults with stroke evaluating electromechanical- or robot-assisted gait training. Stroke could be clinically diagnosed and of any severity, stage or setting. Trials could evaluate any electromechanical or robotic device that enable repetitive walking practice. These are broadly classified into end-effector (where the participants feet are placed on footplates that are moved to simulate walking) or exoskeleton (where a frame is attached to the body segments which move the knees and hips to simulate walking). The Gait Trainer GT and Haptic Walker are examples of end-effector devices. The Lokomat is an example of an exoskeleton device. The comparison for all trials was electromechanical- or robotic-assisted training plus normal care versus normal care alone. Normal care involved over-ground gait training and exercise with a physiotherapist. The primary outcome was the proportion of participants walking independently. Walking independence could be assessed using the Functional Ambulation Category (score 4 or 5), Barthel Index ambulation item (score 3), Functional Independence Measure walking item (score 6 or 7) or Rivermead Mobility Index (‘walking inside, with an aid if necessary’ or ‘walking on uneven ground’ item score ‘yes’). We decided to report one secondary outcome, walking speed, in this summary because we think it is of interest to people with stroke and clinicians. Two reviewers independently selected trials for inclusion, extracted data and evaluated trial quality. Disagreements were resolved by discussion or arbitration from a third reviewer. Trial methodology was evaluated using the Cochrane risk of bias tool and certainty of evidence was evaluated using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. Meta-analysis was used to calculate the odds ratio and its 95% confidence interval (CI) for the ability to walk independently.
62 trials (2,440 participants) were included in the meta-analyses. Participants were aged 47 to 76 years, on average, and about 65% were men. Electromechanical- or robotic-assisted training commonly involved sessions of 30 to 60 minutes in duration on 3 to 5 days/week for 3 to 4 weeks. 24 trials recruited people 3 months or less and 16 recruited people > 3 months post stroke. 40 trials recruited only independent walkers, 18 recruited only dependent walkers, and 4 a mix of independent and dependent walkers. 41 trials used an exoskeleton device and 14 an end-effector device (7 trials could not be categorised as exoskeleton or end-effector).
Electromechanical- or robot-assisted gait training in combination with physiotherapy increased the odds of participants becoming independent in walking by 2.14 (95% CI 1.57 to 2.92; 38 trials; 1,567 participants; high-certainty evidence) and increased walking speed by a mean of 0.06 m/sec (95% CI 0.02 to 0.10; 42 trials; 1,600 participants; low certainty evidence) compared to physiotherapy alone at the end of the intervention phase.
Electromechanical- or robotic-assisted training in combination with physiotherapy increases the chance of regaining independent walking ability after stroke. If 100 people with stroke who could not walk independently received electromechanical- or robotic-assisted training and physiotherapy, about 62 would be able to walk independently at the end of the intervention period compared to 45 in the group receiving physiotherapy alone.
Mehrholz J, et al. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev 2020;Issue 10
Organised inpatient (stroke unit) care for stroke
Stroke is the third leading cause of disability and the second leading cause of mortality worldwide. Stroke units provide guideline-directed and multi-disciplinary care (medical, nursing, and allied health, including physiotherapy) for patients hospitalised with stroke. This systematic review aimed to estimate the effect of stroke unit care compared to an alternate form of inpatient care (conventional care or an alternate model of stroke unit care).
The review performed sensitive searches of 13 databases and trial registers (including Medline, Embase, and Cochrane CENTRAL) plus other strategies (including checking reference lists and contacting trialists) to identify randomised controlled trials that compared stroke unit care with an alternate form of inpatient care for people who had sustained a stroke. Pseudo-randomised trials and cross-over trials were excluded. Any model of stroke unit care was included (dedicated stroke ward, mobile stroke team, mixed rehabilitation ward). The comparator was an alternate form of inpatient care, which could include conventional care in a general medical ward or an alternate model of stroke unit care. A clinical definition of stroke was used, and there were no restrictions based on stroke severity or type, age or sex. The composite outcome of death or dependency or requiring institutional care (termed a “poor outcome”) at the end of scheduled follow-up was the primary outcome. One reviewer screened the titles and abstracts of the search results to exclude obviously irrelevant articles. Two reviewers selected trials for inclusion, extracted data, and evaluated risk of bias and certainty of evidence. Risk of bias was evaluated using the Cochrane risk of bias tool. Certainty of evidence was classified using the Grading of Recommendations Assessment, Development and Evaluation (or GRADE) approach. Meta-analysis was used to estimate the risk of a poor outcome, expressed as an odds ratio and its 95% confidence interval (CI). Four subgroup analyses were performed: (1) age <75 years versus 75 years or older; (2) female versus male; (3) mild versus moderate versus severe stroke, and, (4) ischaemic versus haemorrhagic stroke. Network meta-analysis was used to explore the impact of different models of stroke care, with effect size reported as odds ratios and 95% CIs.
29 trials (5,902 participants) were included in the analyses. 20 trials (4,127 participants) compared stroke unit care with conventional care in a general medical ward, 6 trials (982 participants) compared different models of stroke unit care, and 3 trials (793 participants) incorporated more than one comparison.
There was moderate-certainty evidence that stroke unit care reduced the risk of a poor outcome at the end of scheduled follow-up (median 1 year) compared to conventional care, with an odds ratio of 0.77 (95% CI 0.69 to 0.87; 26 trials; 5,336 participants). This outcome was independent of patient age, sex, stroke severity, and stroke type.
The network meta-analysis revealed that this effect was largest when the model of stroke unit care involved a dedicated stroke ward. Using conventional care in a general ward as the comparator, the odds of a poor outcome were 0.74 (95% CI 0.62 to 0.89; moderate certainty) for dedicated stroke wards, 0.88 (95% CI 0.58 to 1.34; low certainty) for mobile stroke teams, and 0.70 (95% CI 0.52 to 0.95; low certainty) for mixed rehabilitation wards.
Stroke patients who receive stroke unit care are more likely to be alive, independent, and living at home 1 year after the stroke. This benefit was independent of patient age, sex, stroke severity and stroke type, and was most obvious in stroke units based in a discrete stroke ward. For every 100 stroke patients receiving stroke unit care, two extra patients will be alive, six more will be independent, and six more living at home.
Langhorne P, et al. Organised inpatient (stroke unit) care for stroke: network meta-analysis. Cochrane Database Syst Rev 2020;Issue 4
Aerobic exercise interventions reduce blood pressure in patients after stroke or transient ischaemic attack
People who have had a stroke or transient ischaemic attack (TIA) have an increased risk of a second cardiovascular event (eg, stroke, heart attack) and commonly exhibit cardiovascular risk factors (eg, hypertension, diabetes, dyslipidemia). To-date, research on prevention of cardiovascular events and risk factors has focused on drug interventions. The evidence-base of non-drug treatments, particularly exercise, is less clear. The aim of this systematic review was to estimate the average effect of exercise interventions on reducing secondary cardiovascular events or risk factors in people with stroke or TIA.
The inclusion criteria were: recruiting adults who had sustained a stroke or TIA; evaluating exercise interventions; compared to usual care or control conditions; reporting the outcomes of cardiovascular events (including cardiovascular death) and/or cardiovascular risk factors; and, a randomised controlled trial design. Exercise interventions included aerobic, resistance, or a mixture of both aerobic and resistance. Motor training interventions aimed at improving function were only included if they had a substantive aerobic or resistance component. The cardiovascular risk factors evaluated were blood pressure (systolic and diastolic), lipid profile (total, low-density, and high-density cholesterol), fasting plasma glucose, and body mass index. Sensitive searches were performed in 11 databases (including PubMed and China National Knowledge Infrastructure). Two reviewers independently selected the included trials and extracted data, with any disagreements resolved by consensus discussions or arbitration by a third reviewer. The Consensus on Exercise Reporting Template (CERT) was used to evaluate completeness of reporting of the interventions. The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach (that included trial methodological quality evaluated using the Cochrane risk of bias tool) was used to categorise the overall quality of the evidence for each outcome. Meta-analysis was used to calculate the mean effect and 95% confidence interval (CI) for each outcome. Pre-specified subgroup analyses were used to estimate the effects of early (< 6 months) versus late (> 6 months) exercise initiation; incorporation of health education in the intervention; and, participant type (TIA or non-disabling stroke versus severe stroke).
Twenty trials (n = 1,031 participants) were included in the review. Most trials only recruited people with stroke (16 trials; three exclusively recruited people with disabling stroke), initiated the intervention within 6 months of the primary stroke or TIA (11 trials), and compared exercise to usual care (12 trials). Ten trials used aerobic exercise, two used resistance exercise, and eight used a combination of aerobic and resistance exercise. Four trials incorporated health education with the exercise intervention.
Only one small trial (70 participants) reported the cardiovascular events outcome. In this trial exercise reduced the risk of hospitalisation or death due to stroke, myocardial infarction or peripheral arterial disease (adjusted hazard ratio 0.194, 95% CI 0.121 to 0.737) compared to the control group. There was moderate quality evidence that exercise reduced systolic blood pressure (-4 mmHg, 95% CI -7 to -2, 12 trials, 606 participants) but had no effect on fasting glucose (-0.14 mmol/L, 95% CI -0.29 to 0.01, 7 trials, 364 participants) and body mass index (0.00 kg/m2, 95% CI -0.26 to 0.25, 8 trials, 446 participants) compared to control interventions. There was low quality evidence that exercise reduced diastolic blood pressure (-3 mmHg, 95% CI -5 to -1, 12 trials, 606 participants) and total cholesterol (-0.27 mmol/L, 95% CI -0.54 to 0.00, 9 trials, 370 participants) compared to control interventions. There was very low quality evidence that exercise had no effect on low-density (-0.28 mmol/L, 95% CI -0.63 to 0.07, 7 trials, 303 participants) and high-density (0.08 mmol/L, 95% CI -0.02 to 0.17, 9 trials, 394 participants) cholesterol compared to control interventions.
Data from the subgroup analyses were reported for the outcomes of systolic and diastolic blood pressure only. The reduction in systolic blood pressure was most pronounced in trials that initiated the exercise intervention within 6 months of stroke or TIA (< 6 months -8 mmHg, 95% CI -12 to -5, 6 trials, 298 participants; > 6 months -2 mmHg, 95% CI -4 to -1, 6 trials, 308 participants), incorporated an educational component (exercise + education -8 mmHg, 95% CI -14 to -1, 4 trials, 200 participants; exercise only -3 mmHg, 95% CI -4 to -1, 8 trials, 406 participants), and recruited participants with TIA or non-disabling stroke (TIA or non-disabling stroke -5 mmHg, 95% CI -9 to -2, 9 trials 428 participants; disabling stroke -3 mmHg, 95% CI -4 to -1, 3 trials, 178 participants). The reduction in diastolic blood pressure was also more pronounced in trials that initiated the exercise intervention within 6 months of stroke or TIA (< 6 months -3 mmHg, 95% CI -6 to -1, 6 trials, 297 participants; > 6 months -2 mmHg, 95% CI -5 to 1, 6 trials, 309 participants) and recruited participants with TIA or non-disabling stroke (TIA or non-disabling stroke -4 mmHg, 95% CI -5 to -2, 9 trials 428 participants; disabling stroke 1 mmHg, 95% CI 0 to 2, 3 trials, 178 participants). In contrast, the effects on diastolic blood pressure were less pronounced in trials that incorporated an education component (exercise + education -2 mmHg, 95% CI -5 to 1, 4 trials, 200 participants; exercise only -3 mmHg, 95% CI -6 to 0, 8 trials, 406 participants).
Aerobic and/or exercise can result in reductions in some cardiovascular risk factors (systolic and diastolic blood pressure, total cholesterol) in people with stroke or TIA, particularly if initiated early, provided alongside education, and targeting people with TIA and non-disabling stroke. Investigating the effects of exercise on preventing cardiovascular events is a future research priority.
Wang C, et al. Aerobic exercise interventions reduce blood pressure in patients after stroke or transient ischaemic attack: a systematic review and meta-analysis. Br J Sports Med 2019;53(24):1515-25.
Supervised lifestyle intervention for people with metabolic syndrome improves outcomes and reduces individual risk factors of metabolic syndrome
The objective of this systematic review were to determine the effectiveness of lifestyle interventions on the prevalence of metabolic syndrome and on independent, modifiable risk factors for metabolic syndrome in people with metabolic syndrome. Randomised controlled trials published in English that evaluated the effectiveness of supervised, multifaceted lifestyle interventions in people with metabolic syndrome were included. Lifestyle interventions were defined as any supervised intervention involving both diet and exercise with or without other components, such as counselling. The risk of bias of the included trials was assessed using the PEDro scale, and these were used to determine the quality of the evidence using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. Outcomes were prevalence of metabolic syndrome, risk factors for metabolic syndrome (eg, waist circumference, triglycerides, systolic blood pressure, body mass index), and quality of life. Adverse events were a secondary outcome.
15 articles reporting the results for 10 trials were included (n = 1,160 participants). Compared to usual care, there was moderate quality evidence that lifestyle interventions reduced the prevalence of metabolic syndrome (risk ratio 0.61, 95% confidence interval (CI) 0.38 to 0.96, 4 trials, 463 participants). There was moderate quality evidence that lifestyle interventions reduce waist circumference (mean difference -4.9 cm, 95% CI -8.0 to -1.7, 6 trials, 643 participants), low quality evidence that lifestyle interventions reduce triglycerides (standardised mean difference -0.46, 95% CI -0.88 to -0.04, 9 trials, 797 participants) and systolic blood pressure (mean difference -6.5 mmHg, 95% CI -10.7 to -2.3, 8 trials, 689 participants), and very low quality evidence that lifestyle interventions reduce body mass index (standardised mean difference -1.30, 95% CI -2.18 to -0.44, 9 trials, 798 participants). There was no difference for quality of life (standardised mean difference 1.68, 95% CI -0.23 to 3.58, 4 trials, 225 participants) and no trials reported adverse events.
Very low to moderate quality evidence supports the use of multifaceted, supervised lifestyle interventions to reduce the prevalence of metabolic syndrome and to reduce risk factors for this condition.
van Namen M, et al. Supervised lifestyle intervention for people with metabolic syndrome improves outcomes and reduces individual risk factors of metabolic syndrome: a systematic review and meta-analysis. Metabolism 2019;101:153988
Exercise therapy for functional capacity in chronic diseases
This umbrella review included 85 meta-analyses of randomised controlled trials evaluating the effectiveness of exercise therapy on functional capacity in people with chronic disease. Exercise therapy was compared with no treatment or usual care in adults with non-communicable chronic diseases defined by the World Health Organisation (WHO). The methodological quality of the included meta-analysis was evaluated using the AMSTAR checklist. The type of exercise therapy was classified into four categories: aerobic exercise, resistance training, aerobic and resistance training combined, and other condition-specific exercise-based training. The authors conclude that exercise therapy was effective for improving physical performance and functional capacity in all included chronic diseases (Alzheimer’s disease, cancer, chronic fatigue syndrome, chronic heart failure, chronic kidney disease, chronic obstructive pulmonary disease, cognitive impairment, coronary heart disease, dementia, fibromyalgia, interstitial lung disease, multiple sclerosis, osteoarthritis, Parkinson’s disease, peripheral arterial disease, rheumatoid arthritis, stroke, and type 2 diabetes). Around half of the effect estimates were of moderate to large magnitude and likely to be clinically important. Results were mostly similar among the different types of exercises, except for condition-specific programs that had a lower proportion of significant results compared with the others. Exercise also appears to be safe, but adverse events were not consistently reported. Exercise therapy should be recommended for people with chronic disease to improve functional capacity and reduce disability.
Pasanen T et al. Exercise therapy for functional capacity in chronic diseases: an overview of meta-analyses of randomised controlled trials. Br J Sports Med 2017;51:1459-65
Exercise to prevent falls in older adults
In this updated review, the authors included 88 trials (n=19,478 participants) which tested the effect of exercise to prevent falls in older people. Exercise reduced the rate of falls in community dwelling older people by 21% (pooled rate ratio 0.79, 95% CI 0.73 to 0.85, p<0.001, 69 comparisons). Greater effects were observed with balance training and that least 3 hours per week of exercise (39% reduction in falls). Exercise reduced the rate of falls in people with Parkinson’s disease by 53% (pooled rate ratio 0.47, 95% CI 0.30 to 0.73, p=0.001, 6 comparisons) and by 45% in people with cognitive impairment (pooled rate ratio 0.55, 95% CI 0.37 to 0.83, p=0.004, 3 comparisons). There was no significant effect of exercise for preventing falls in people after stroke (pooled rate ratio 0.74, 95% CI 0.42 to 1.32, p=0.31, 3 comparisons), in people recently discharged from hospital (pooled rate ratio 1.16, 95% CI 0.88 to 1.52, p=0.30, 3 comparisons), and in residential care settings (pooled rate ratio 0.90, 95% CI 0.72 to 1.12, p=0.35, 15 comparisons). Most of the interventions conducted in the included studies involved exercise prescribed as a single intervention by trained health professionals, or professionals specialising in exercise, to minimise the risk of harm during the program. Exercise as a single intervention can prevent falls in community-dwelling older people.
Sherrington C et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med 2017;51(24):1750-8
Interventions involving repetitive practice improve strength after stroke
This systematic review evaluates the effects of interventions involving repetitive practice on strength and activity in people with stroke. Randomised controlled trials conducted in adult participants with a diagnosis of stroke (acute or chronic) compared to a sham or no intervention were included. The primary outcome of this review was strength. The secondary outcomes were activity of the affected upper and lower limb. Risk of bias was assessed with the Cochrane risk of bias tool. In total, 52 studies were included, with 46 studies (n = 1928) in the meta-analysis for strength. Interventions included task-specific training, electromyography-triggered functional movement, robotics, constrained-induced movement therapy, Bobath, cycling, assistive technology, video games, whole body vibration, mirror therapy, and water-based exercises. The overall standardised mean difference of repetitive practice on strength when the upper and lower limb studies were combined was 0.25 (95% CI 0.16 to 0.34). The most common intervention was task-specific training (18 studies, 931 participants) had a standardised mean difference of 0.21 (95% CI 0.08 to 0.34) on strength. The intervention with the largest effect on strength was constraint-induced movement therapy (2 studies, 22 participants), with a standardised mean difference of 1.49 (95% CI 0.44 to 2.54). Twenty-four studies (n = 912 participants) investigated the effects of repetitive practice on upper limb activity, with repetitive practice being superior to control conditions (standardised mean difference 0.15, 95% CI 0.02 to 0.29). Larger effects were observed for repetitive practice on lower limb activity (20 studies, 952 participants), with a standardised mean difference of 0.25 (95% CI 0.12 to 0.38). Interventions involving repetitive practice improve strength after stroke, and the improvement in strength is accompanied by improvements in activity.
De Sousa et al. Interventions involving repetitive practice improve strength after stroke: a systematic review. J Physiother 2018;64(4):210-21
Mirror therapy for improving motor function after stroke
This recently updated Cochrane systematic review evaluates the effects of mirror therapy on motor function, pain and visuospatial neglect in people with stroke. Randomised controlled trials and crossover trials comparing mirror therapy with no treatment, sham therapy and other interventions were included. Interventions that used direct mirroring of movement in any format were included. Studies that combined mirror therapy with other interventions were included if at least 50% of the total intervention was mirror therapy. The primary outcome was motor function measured with any scale. Upper limb motor function was prioritised over lower limb motor function. Secondary outcomes were measures of motor impairment, pain and visuospatial neglect. A total of 62 studies (n=1982 participants) were included (57 randomised controlled trials, 5 crossover trials). Mirror therapy was provided three to seven times per week, for between 15 and 60 minutes in each session and for a duration of 2 to 8 weeks. Compared to other interventions, mirror therapy significantly improved motor function at the end of the treatment phase (standardised mean difference 0.47, 95% CI 0.27 to 0.67, 1173 participants from 36 trials, moderate quality evidence). However, these benefits of mirror therapy on motor function did not appear to persist 6 months after the end of treatment (standardised mean difference 1.20, 95% CI -0.78 to 3.18, 88 participants from 2 trials). Mirror therapy significantly improved motor impairment (standardised mean difference 0.49, 95% CI 0.32 to 0.66, 1291 participants from 39 trials, moderate quality evidence) and reduced pain (standardised mean difference -0.89, 95% CI -1.67 to -0.11, 248 participants from 6 trials, low quality evidence) at the end of the treatment phase when compared to other treatments. Mirror therapy was no better than other treatments for improving visuospatial neglect (standardised mean difference 1.06, 95% CI -0.10 to 2.23, 175 participants from 5 trials, low quality evidence). There was uncertainty around some effect estimates due to small samples in the included trials. Future trials with larger sample sizes are likely to increase the precision of the estimates reported in this review.
Thieme H et al. Mirror therapy for improving motor function after stroke. Cochrane Database Syst Rev 2018;Issue 7
Circuit class therapy for improving mobility after stroke
In this review, the authors included 17 trials (n=1,297 participants) which evaluated the effects of circuit class rehabilitation compared to usual care or sham rehabilitation for people after stroke of any type, severity and stage. Circuit class therapy was defined as physical rehabilitation in a group environment, with no more than one staff member per three patients. One circuit class per week for four weeks was the minimum dosage required for inclusion in the review. Only studies reporting interventions that focused on repetitive practice of functional tasks arranged in a circuit with the aim of improving mobility, were included. Ten studies (835 participants) measured walking capacity (Six-Minute Walk Test) demonstrating that circuit class therapy was superior to other interventions (mean difference (MD) 60.86 m, 95% confidence interval (CI) 44.55 to 77.17). Eight studies (744 participants) measured gait speed, again finding in favor of circuit class therapy compared with other interventions (MD 0.15 m/s, 95% CI 0.10 to 0.19). Circuit class therapy also demonstrated superior effects in other aspects of walking and balance (Timed Up and Go: five studies, 488 participants, MD -3.62 seconds, 95% CI -6.09 to -1.16; Activities of Balance Confidence scale: two studies, 103 participants, MD 7.76, 95% CI 0.66 to 14.87). There was low quality of evidence that no adverse events (e.g., falls during therapy) are associated with circuit class therapy. There is moderate quality evidence that circuit class therapy provides a clinically important benefit in mobility for people after stroke. More studies investigating quality of life and cost-benefits are needed.
English C et al. Circuit class therapy for improving mobility after stroke. Cochrane Database Syst Rev 2017;Issue 6.
Repetitive task training for improving functional ability after stroke
In this Cochrane review, the authors included 33 randomised controlled trials, involving 1,853 adults who have suffered a stroke. Trials of repetitive task training were considered eligible if the RRT intervention comprised an active motor sequence performed repetitively within a single training session, and where the practice was aimed towards a clear functional goal (eg, picking up a cup, sit-to-stand). Eligible control interventions were usual care or placebo. In many studies risk of bias was unclear due to poor reporting of study details. The quality of evidence was limited by inconsistency of results across studies, small sample sizes, and poor reporting. Therefore, the available evidence was only of ’moderate’ or ’low’ quality according to the GRADE system.
The review concluded that there was low-quality evidence that repetitive task training improves arm function (standardised mean difference (SMD) 0.25, 95% confidence interval (CI) 0.01 to 0.49; 11 studies, n=749), hand function (SMD 0.25, 95% CI 0.00 to 0.51; 8 studies, n=619), and lower limb functional measures (SMD 0.29, 95% CI 0.10 to 0.48; 5 trials, n=419). There was moderate-quality evidence that repetitive task training improves walking distance (mean difference (MD) 34.80, 95% CI 18.19 to 51.41; 9 studies, n=610) and functional ambulation (SMD 0.35, 95% CI 0.04 to 0.66; 8 studies, n=525). Improvements for both upper and lower limb function were sustained up to six months post treatment. The effect estimates were not altered by intervention type, dosage of task practice or time since stroke.
French B, et al. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst Rev 2016;Issue 11