Return to all evidence summaries
Oncology
Oncology includes papers evaluating interventions for health problems due to tumours or cancers.
The most recently synthesised review is at the top of the list.
- Cardiovascular training for fatigue in people with cancer
- Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer
- Effectiveness of exercise training on cancer-related fatigue in colorectal cancer survivors
- Motivational strategies to improve adherence to physical activity in breast cancer survivors
- Efficacy of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery
- Moderators of exercise effects on cancer-related fatigue
- Exercise therapy for functional capacity in chronic diseases
- Effects of physical exercise after treatment of early breast cancer
- Exercise improves quality of life in patients with cancer
Cardiovascular training for fatigue in people with cancer
Cancer-related fatigue is the most common and severe symptom of cancer and cancer treatment. Prevalence ranges between 50 to 90% and is associated with decreased quality of life. This systematic review aimed to estimate the effects of cardiovascular training compared to no training on fatigue and quality of life in people with cancer.
Articles were included if they were randomised controlled trials evaluating cardiovascular training in people with cancer, study samples had 20 or more per group, had at least 80% of participants aged 18 years or older with any diagnosed type and stage of cancer and any type of anti-cancer therapy; intervention was at least five sessions of structured cardiovascular exercise (i.e. aerobic training) with face-face instruction (either in person or via video). The comparator was no intervention, a minimally active intervention (e.g. progressive muscle relaxation) or usual care. Eight databases (including Cochrane Central Register of Controlled Trials, Medline and PEDro), two clinical trial registries and citation tracking were searched between 2003 and 2023. Primary outcomes were cancer-related fatigue using MFI, FACT-F or FBI and quality of life using EORTC QLQ-C30 or FACT-G. At least two reviewers independently determined eligibility, extracted data and assessed risk of bias. Disagreements were resolved through arbitration by a third reviewer. Treatment effects were quantified by calculating mean differences (MD) or standardised mean differences (SMD), both with 95% confidence intervals. The overall certainty of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Twenty-three trials (2,135 participants) were included. The most frequent cancer diagnosis was breast cancer (57%), followed by lung (7%) and prostate (6%) cancers, ranging from Stages I to IV. Excluding studies of breast, prostate and testicular cancer, the proportion of females ranged from 27% to 100%, and the mean age ranged from 44 to 66 years. Ten trials initiated cardiovascular training during anti-cancer therapy, 13 after completing anti-cancer therapy and none before commencing anti-cancer therapy. There was a large range of exercise prescription, though the most common was individual, supervised sessions involving cycling and walking at moderate-high intensity (range low-moderate to high intensity) for three times per week (range one to five times), with a training duration of eight to 12 weeks (range three to 26 weeks).
During anti-cancer therapy, there was moderate-certainty evidence that cardiovascular training reduces cancer-related fatigue slightly in the short-term, up to 12 weeks post-intervention (6 studies, 593 participants; SMD -0.27, 95%CI -0.43 to -0.11); and has little to no difference in quality of life (6 studies, 612 participants; SMD -0.17, 95%CI -0.33 to -0.01). In the medium-term (12 to 26 weeks) and long-term (26 weeks+) post-intervention, there was very low-certainty evidence that cardiovascular training had an effect on cancer-related fatigue (1 study, 62 participants; MD 2.67, 95% CI -2.58 to 7.92; and 2 studies, 230 participants; SMD -0.04, 95% CI -0.33 to 0.22, respectively) and quality of life (1 study, 62 participants; MD 6.79, 95% CI -4.39 to 17.97; and 2 studies, 230 participants; SMD -0.08, 95% CI -0.34 to 0.18, respectively).
After anti-cancer therapy, there was very low-certainty evidence that cardiovascular training had an effect on cancer-related fatigue (6 studies, 497 participants; SMD -0.37, 95% CI -0.73 to 0.00) and quality of life (8 studies, 642 participants; SMD -0.27, 95% CI -0.54 to 0.01). In the long-term post-intervention (26 weeks+), there was very low-certainty evidence cardiovascular training had an effect on cancer-related fatigue after anti-cancer therapy (2 studies, 262 participants; SMD -0.43, 95C%CI -0.93 to 0.07) and quality of life (1 study, 201 participants; MD 3.10, 95%CI -1.12 to 7.32).
Cardiovascular training during anti-cancer therapy slightly reduces short-term cancer-related fatigue and has little to no effect on short-term quality of life (moderate-certainty evidence); whereas the effects on medium- and long-term fatigue and quality of life are uncertain. The effects of cardiovascular training after anti-cancer therapy on short- and long-term fatigue and quality of life are uncertain.
Wagner C, Ernst M, Cryns N, Oeser A, Messer S, Wender A, Wiskemann J, Baumann FT, Monsef I, Bröckelmann PJ, Holtkamp U, Scherer RW, Mishra S and Skoetz N. Cardiovascular training for fatigue in people with cancer. Cochrane Database of Systematic Reviews. 2025: Issue 2, Art No: CD015517; doi: 10.1002/14651858.CD015517.

Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer
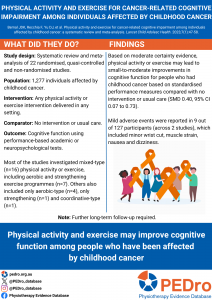
Individuals affected by childhood cancer may experience long-term cognitive impairments. Although exercise has been recommended for other cancer-related symptoms, the effect of physical activity on cognitive functioning in those affected by childhood cancer remains unknown. This systematic review aimed to estimate the effects of physical activity interventions compared to no intervention or usual care on cognitive function in people affected by childhood cancer.
Seven electronic databases were searched for randomised (RCTs) and quasi-randomised controlled trials, and non-randomised studies of interventions (NRSIs). There were no language or date restrictions. Eligible studies included individuals diagnosed with cancer at age 0-19 who received or are receiving cancer treatment. The intervention could be any frequency, intensity, volume, duration, or type of exercise or physical activity and delivered in any setting (e.g., gym). Control participants either had no treatment or usual care. The primary outcome of interest was performance on any standardised and objective academic or neuropsychological test of cognitive function. Outcomes related to cognitive function were categorised into 6 domains: complex attention, executive function, learning and memory, language, perceptual-motor function, and social cognition. Two independent reviewers screened for eligible studies, data extraction, assessment of risk of bias and certainty of evidence. Risk of bias was assessed using the Cochrane Risk of Bias Tool 2 for randomised and quasi-randomised controlled trials. Certainty of evidence was assessed for each outcome using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. A meta-analysis pooled all trials using a random-effects model to estimate the standardised mean difference (Hedges’ g) between the intervention and control conditions at the end of the intervention period. A composite score was calculated for each study to determine the overall intervention effect on general cognitive performance, which was used in the meta-analysis of the primary outcome.
Twenty-two studies were included in the review (n = 1,277). The median age at recruitment was 12 years (IQR 11-14), and the median time since treatment completion was 2.5 years (IQR -1.1-3.0). Interventions included aerobic, strengthening, and/or coordination-based exercises, with a median period of 12 weeks (IQR 10.24). Sessions lasted a median duration of 45 minutes (IQR 40-60) across a median of 3 days/week (IQR 2.5-5.0). Adverse events were reported in two studies, of which nine events were noted (minor wrist cut, muscle strain, nausea, vomiting, drop in systolic blood pressure, dizziness, and nosebleed).
Five randomised controlled trials (n = 245) were included in the meta-analysis of the primary outcome. No RCT in the primary outcome meta-analysis was considered high risk of bias. There was moderate certainty evidence that physical activity resulted in small-to-moderate improvements in objective tests of cognitive function compared with control (SMD 0.40, 95% CI 0.07 to 0.73).
Physical activity and exercise interventions improve cognitive function in people who had childhood cancer. Future research should explore the optimal frequency, intensity, volume, duration, and type of physical intervention across different patient characteristics (e.g., type of cancer) for improving cognitive function.
Bernal JDK, Recchia F, Yu DJ, et al. Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer: a systematic review and meta-analysis. Lancet Child Adolesc Health. 2023;7(1):47-58. doi:10.1016/S2352-4642(22)00286-3
Effectiveness of exercise training on cancer-related fatigue in colorectal cancer survivors
Colorectal cancer is the third most commonly diagnosed cancer worldwide. Up to half of colorectal cancer survivors report cancer-related fatigue, a debilitating and often long-term symptom impacting health-related quality of life and activity participation. . Exercise training is recommended in clinical guidelines for the management of cancer-related fatigue, but the evidence is largely from studies involving people with breast cancer or where exercise has been combined with other interventions, such as nutrition counselling. This review aimed to estimate the effects of exercise training compared to non-exercise training usual care on cancer-related fatigue in survivors of colorectal cancer, during chemotherapy and following completion of treatment.
The protocol was prospectively registered. Five databases (including PEDro and PubMed) were searched for randomised controlled trials published in English. Participants were adult colorectal cancer survivors (with survivorship defined as commencing from the time of diagnosis). The intervention was exercise training alone, defined as structured physical activity to improve or maintain physical condition. The comparator was no exercise training. Self-reported fatigue intensity was the outcome of interest. Two independent reviewers selected trials for inclusion, evaluated risk of bias and extracted data. Any disagreements were resolved by a third reviewer. Risk of bias was evaluated using the PEDro scale. Certainty of evidence was rated using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach. A meta-analysis pooled the included trials to calculate standardised mean differences, 95% confidence intervals (CI) and 95% prediction intervals (PI) to estimate the interval within which a future treatment effect would fall. One subgroup analysis was planned to compare differences in participants receiving chemotherapy compared to participants who were post-treatment.
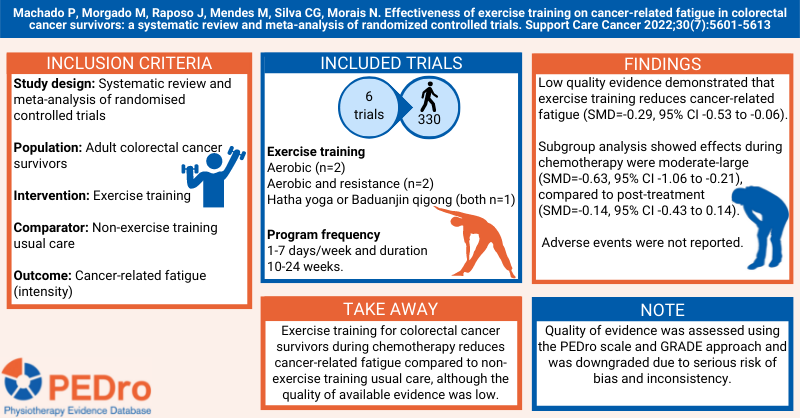
Six trials, involving 330 participants were included (n=170 intervention, n=160 usual care). All participants had stage I-III (non-metastatic) disease. Three trials (n=156) were conducted after treatment, two during adjuvant chemotherapy (n=120) and one predominantly after treatment (n=54 of which 3.7% were receiving chemotherapy). Two trials included aerobic exercise alone, two aerobic and resistance, one trial Hatha yoga (slow pace with breathing control and stretching) and one Baduanjin Qigong (physical postures and movements, combined with mind and breathing exercises). Exercise was home-based in three trials. The program frequency ranged from 1-7 days/week and the duration was between 10-24 weeks.
Four different questionnaires were used to report cancer-related fatigue intensity meaning results were combined as standardised mean differences (SMD) and 95% confidence intervals (CI). On average, participants in the exercise training group reported reduced cancer-related fatigue compared to participants who received non-exercise training usual care (SMD=-0.29, 95% CI -0.53 to -0.06; prediction interval=−0.63; 0.04). Evidence was rated as low quality due to high risk of bias and inconsistency. Subgroup analysis showed effects during chemotherapy were moderate-large (SMD=-0.63, 95% CI -1.06 to -0.21, n=120), whereas effects were uncertain in the post-treatment phase (SMD=-0.14, 95% CI -0.43 to 0.14; prediction interval=−0.76 to 0.47, n=180). Adverse events were not reported.
Exercise training for colorectal cancer survivors during chemotherapy reduces cancer-related fatigue compared to non-exercise training usual care, although the quality of available evidence was low. Further evidence is required regarding the effects of exercise training on cancer-related fatigue in the post-treatment phase.
Machado P, Morgado M, Raposo J, Mendes M, Silva CG, Morais N. Effectiveness of exercise training on cancer-related fatigue in colorectal cancer survivors: a systematic review and meta-analysis of randomized controlled trials. Support Care Cancer. 2022 Jul;30(7):5601-5613. https://doi.org/10.1007/s00520-022-06856-3
Motivational strategies to improve adherence to physical activity in breast cancer survivors
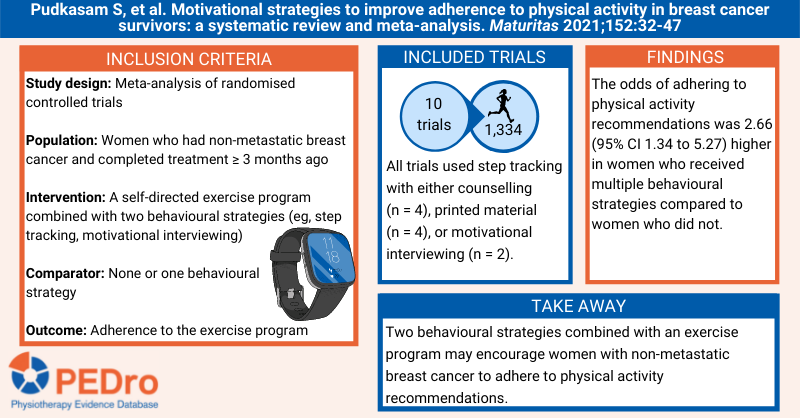
Breast cancer is the leading cause of cancer morbidity and mortality in women globally. Self-directed physical activity or exercise programs are associated with positive breast cancer outcomes. Behavioural strategies that can increase adherence with these programs include self-monitoring by using a step tracking device and motivational interviewing. This systematic review aimed to estimate the effect of different behavioural strategies to improve adherence to self-directed physical activity or exercise programs in women who had non-metastatic breast cancer.
Guided by a prospectively registered protocol, sensitive searches were performed in six databases (including PubMed and Cochrane CENTRAL) to identify randomised controlled trials evaluating self-directed physical activity or exercise programs in women with non-metastatic breast cancer. Participants must have completed surgery, chemotherapy, and radiotherapy treatments for stage 0 to III breast cancer at least 3 months prior to recruitment. The intervention was any form of self-directed physical activity or exercise program (ie, at least half the program was implemented without supervision from a health professional). Behavioural strategies used in the programs were classified as step tracking and counselling, step tracking and motivational interviewing, and step tracking and printed material. The comparator was usual care. The primary outcome was adherence at the end of follow-up measured as a dichotomous (percentage achieving an exercise volume recommendation – full or partial adherence with the program or a physical activity recommendation) or continuous (measures of exercise duration, intensity, or step count) variable. Two reviewers independently selected trials for inclusion, with any disagreements resolved by a third reviewer. Data were extracted by one reviewer and verified by up to two other reviewers. Two reviewers evaluated risk of bias using the Cochrane risk of bias tool, with any disagreements resolved by discussion. Certainty of evidence was not evaluated. Meta-analysis was used to pool the included trials, using odds ratios and 95% confidence intervals (CI) for dichotomous variables, and standardised mean difference and 95% CIs for continuous variables. Trials in the meta-analysis were grouped according to the behavioural strategies used: step tracking and counselling, step tracking and motivational interviewing, and step tracking and printed material.
Ten trials (1,334 participants) with a follow-up of between 12 weeks and 6 months were included in the meta-analyses. The mean age of women in the trials was 50-62 years. Four trials used step tracking and counselling, two used step tracking and motivational interviewing, and four used step tracking and printed material, in conjunction with a self-directed physical activity or exercise program. Comparator groups received usual care, waitlist control or step tracking.
More participants achieved a physical activity recommendation in groups receiving behavioural strategies in combination with self-directed exercise (218/474, 46%) than in control conditions (152/477, 32%), with an odds ratio 2.66 (95% CI 1.34 to 5.27; 6 trials; 951 participants). This effect was slightly larger for step tracking and counselling (odds ratio 7.10; 95% CI 1.13 to 44.75; 3 trials; 373 participants) and step tracking and motivational interviewing (odds ratio 5.95; 95% CI 2.29 to 15.44; 1 trial; 87 participants) than for step tracking and printed material (odds ratio 1.24; 95% CI 0.72 to 2.13; 2 trials; 491 participants). The outcomes of full or partial adherence with the program were not reported.
Participants in groups receiving behavioural strategies in combination with self-directed exercise achieved 0.55 standard deviations more moderate to vigorous physical activity than those in control conditions (95% CI 0.30 to 0.79; 9 trials; 1,262 participants). This effect was consistent across the step tracking and counselling (standardised mean difference 0.70; 95% CI 0.14 to 1.25; 4 trials; 435 participants), step tracking and motivational interviewing (standardised mean difference 0.70; 95% CI 0.39 to 1.01; 2 trials; 167 participants), and step tracking and printed material (standardised mean difference 0.32; 95% CI 0.07 to 0.57; 3 trials; 660 participants) subgroups.
When combined with a self-directed physical activity or exercise program, the behavioural strategies of step tracking with counselling, motivational interviewing or printed material appear to increase adherence with physical activity in women who had non-metastatic breast cancer.
Pudkasam S, et al. Motivational strategies to improve adherence to physical activity in breast cancer survivors: a systematic review and meta-analysis. Maturitas 2021;152:32-47
Efficacy of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery
Prehabilitation aims to promote physical and psychological health and address modifiable risk factors prior to surgery to improve postoperative outcomes. There are conflicting results regarding the effectiveness of prehabilitation in patients with cancer awaiting surgery, and the optimal approach to delivering prehabilitation is unclear. This systematic review aimed to estimate the effects of exercise prehabilitation compared to standard care on postoperative outcomes in adults undergoing surgery for abdominal cancer.
Guided by a prospectively registered protocol, citation tracking and sensitive searches were conducted in 5 databases (including Medline and PEDro) to identify (pseudo-)randomised controlled trials that investigated the effects of exercise prehabilitation for adults scheduled to undergo abdominal surgery for cancer. Exercise prehabilitation could involve any form of exercise (including whole body or respiratory exercise) plus education and be delivered either as a stand-alone intervention (ie, unimodal) or included within a framework of multimodal interventions (ie, with nutritional or psychological interventions). The comparator was not exposed to a prehabilitation program, like standard care or no intervention. The outcomes included functional capacity (eg, 6-Minute Walk Test), cardiorespiratory fitness (eg, VO2peak), postoperative complications, hospital length of stay, hospital re-admission, and postoperative mortality, but the primary outcome was not identified. The Consensus Exercise Reporting Template was used to extract information about the interventions. Risk of bias of the included trials was evaluated using version 2 of the Cochrane risk of bias tool. Two reviewers independently selected trials for inclusion, extracted data and evaluated risk of bias. Disagreements were resolved by consensus or by arbitration from a third reviewer. Meta-analyses were performed for each outcome, calculating the mean differences (when data were reported for the same scale), standardised mean differences (when data were reported using different scales) or odds ratios (for dichotomous variables) and their associated 95% confidence intervals (CI). Certainty of evidence was evaluated using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. Three subgroup comparisons were pre-planned: low vs. high functional capacity at baseline; shorter vs. longer prehabilitation programs; and, unimodal vs. multimodal programs.
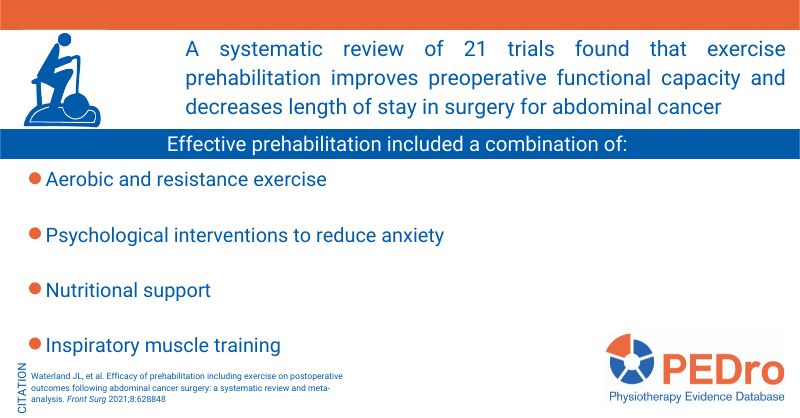
21 trials (1,640 participants) were included in the meta-analysis. Most trials were from Canada (5) or the United Kingdom (5). The type of cancer was colorectal (7 trials), gastro-oesophageal (4), urological (4), other specific cancer (3) or a variety of cancers (3). 9 trials evaluated unimodal exercise prehabilitation and 12 were multimodal. Exercise involved aerobic and strength training (9 trials), aerobic training (5), aerobic, strength and respiratory training (4), respiratory training (2) or education (1). Intervention was commonly provided in a home-based setting by physiotherapists. The frequency and duration of programs generally ranged from five sessions over 1 week to three times/week for 8 weeks.
Compared to standard care, prehabilitation increased preoperative functional capacity by 34 metres on the 6-Minute Walk Test (95% CI 19 to 49; 522 participants; 8 trials; moderate certainty) and reduced postoperative hospital length of stay by a mean of 3.7 days (0.9 to 6.4; 458 participants; 4 trials; moderate certainty). In contrast, there was no difference between standard care and prehabilitation for preoperative cardiorespiratory fitness (mean difference for VO2peak 1.7 ml/min/kg; -0.0 to 3.5; 121 participants; 3 trials; low certainty), postoperative complications (odds ratio 0.81, 95% CI 0.55 to 1.18; 917 participants; 16 trials; low certainty), hospital re-admission (odds ratio 1.07, 0.61 to 1.90; 464 participants; 6 trials; moderate certainty), and postoperative mortality (odds ratio 0.95; 95% CI 0.43 to 2.09; 901 participants; 7 trials; low certainty).
Subgroup comparison was possible for unimodal vs. multimodal programs for functional capacity (6-Minute Walk Test). Compared to standard care, multimodal programs increased the distance walked in 6 minutes by a mean of 33 metres (95% CI 18 to 49; 464 participants; 6 trials) compared to 52 metres (-13 to 116; 58 participants; 2 trials) for unimodal programs. However, this finding should be interpreted with caution because of the small number of participants and trials available for unimodal programs.
Exercise prehabilitation, particularly multimodal approaches, improves preoperative functional capacity and reduces postoperative hospital length of stay in people undergoing surgery for abdominal cancer.
Waterland JL, et al. Efficacy of prehabilitation including exercise on postoperative outcomes following abdominal cancer surgery: a systematic review and meta-analysis. Front Surg 2021;8:628848
Moderators of exercise effects on cancer-related fatigue
This systematic review of individual patient data investigated the effects of exercise on cancer-related fatigue and moderators of exercise interventions. Randomised controlled trials in the Predicting OptimaL cAncer Rehabilitation and Supportive care (POLARIS) database were included in the review if they reported fatigue outcomes. All principal investigators from the trials in the POLARIS database provided individual patient data under a data sharing agreement. The methodological quality of each trial was assessed using the Cochrane risk of bias tool. The main outcome was fatigue after completion of the exercise intervention measured using any scale. Potential moderators of treatment effect were based on previous trials and meta-regression analyses and included age, sex, marital status, education level, body mass index, cancer type, treatment type (surgery, chemotherapy, radiotherapy, hormone therapy), and presence of distant metastases. Characteristics of the exercise programs, including frequency, intensity, type, supervision, session time and volume, were also explored as moderators.
Thirty-one trials (n = 4,366 participants) were included. Of these, 2,437 participants were randomised to an exercise intervention group, and 1,929 to a control group. All trials were conducted in high-income countries, including the Netherlands, United States, Australia, Canada, Germany, United Kingdom and Norway.
Exercise reduced fatigue compared to control (effect size -0.17; 95% confidence interval (CI) -0.22 to -0.12). None of the demographic or clinical characteristics of individual participants moderated the effects of the intervention on fatigue. Compared to control, supervised exercise had larger effects on fatigue than unsupervised exercise interventions (effect size -0.18; 95% CI -0.28 to -0.08). Within supervised interventions, those with a duration of up to 12 weeks showed the larger effects (effect size -0.29; 95% CI -0.39 to -0.20) than those with a duration longer than 24 weeks (effect size -0.11; 95% CI -0.22 to 0.00). No other exercise-related characteristics were identified as moderators of supervised exercise interventions. Within unsupervised interventions, neither duration nor exercise-related characteristics moderated the effect of exercise interventions on fatigue.
Exercise interventions reduce fatigue across all subgroups of patients and types of cancer, supporting a role for exercise in clinical practice for people with cancer. The strongest effects on fatigue were noted in supervised exercise interventions with a duration of up to 12 weeks.
van Vulpen JK et al. Moderators of exercise effects on cancer-related fatigue: a meta-analysis of individual patient data. Med Sci Sports Exerc 2020;52(2):303-14
Exercise therapy for functional capacity in chronic diseases
This umbrella review included 85 meta-analyses of randomised controlled trials evaluating the effectiveness of exercise therapy on functional capacity in people with chronic disease. Exercise therapy was compared with no treatment or usual care in adults with non-communicable chronic diseases defined by the World Health Organisation (WHO). The methodological quality of the included meta-analysis was evaluated using the AMSTAR checklist. The type of exercise therapy was classified into four categories: aerobic exercise, resistance training, aerobic and resistance training combined, and other condition-specific exercise-based training. The authors conclude that exercise therapy was effective for improving physical performance and functional capacity in all included chronic diseases (Alzheimer’s disease, cancer, chronic fatigue syndrome, chronic heart failure, chronic kidney disease, chronic obstructive pulmonary disease, cognitive impairment, coronary heart disease, dementia, fibromyalgia, interstitial lung disease, multiple sclerosis, osteoarthritis, Parkinson’s disease, peripheral arterial disease, rheumatoid arthritis, stroke, and type 2 diabetes). Around half of the effect estimates were of moderate to large magnitude and likely to be clinically important. Results were mostly similar among the different types of exercises, except for condition-specific programs that had a lower proportion of significant results compared with the others. Exercise also appears to be safe, but adverse events were not consistently reported. Exercise therapy should be recommended for people with chronic disease to improve functional capacity and reduce disability.
Pasanen T et al. Exercise therapy for functional capacity in chronic diseases: an overview of meta-analyses of randomised controlled trials. Br J Sports Med 2017;51:1459-65
Effects of physical exercise after treatment of early breast cancer
This recent systematic review evaluates the effects of exercise on body composition, quality of life and survival in women after treatment of early-stage breast cancer (stage I to III). Randomised controlled trials evaluating exercise programs after the end of adjuvant treatment were included. Exercise programs could be counselling or structured, supervised or individualised. The primary outcomes were overall survival and disease-free survival. Secondary outcomes were weight loss, body mass index, waist-hip ratio, body fat, and quality of life. The review identified 60 randomised controlled trials (6,303 participants), with structured or individualised exercise being the most common types of exercise evaluated. Only one trial had data for the primary outcomes and suggested that 8 months of exercise reduced overall mortality compared to usual care (hazard ratio 0.45, 95% CI 0.21 to 0.97), but had no effect on disease-free survival (hazard ratio 0.66, 95% CI 0.38 to 1.17). There was low-quality evidence that exercise reduced body mass index (mean difference 0.89kg, 95% CI 0.28 to 1.5) and percentage body fat (mean difference 1.6%, 95% CI 0.88 to 2.31). There was very low-quality evidence that exercise reduced weight (mean difference 1.36kg, 95% CI 0.21 to 2.51), general quality of life (standardised mean difference 0.45, 95% CI 0.2 to 0.69), physical aspects of quality of life (standardised mean difference 0.51, 95% CI 0.23 to 0.79), and mental aspects of quality of life (standardised mean difference 0.28, 95% CI 0.06 to 0.5). This review highlighted the need for more well-designed and large-scale randomised controlled trials to evaluate the effects of exercise on mortality outcomes.
Soares Falcetta F, et al. Effects of physical exercise after treatment of early breast cancer: systematic review and meta-analysis. Breast Cancer Res Treat 2018;170(3):455-76
Exercise improves quality of life in patients with cancer
In this review, the authors included 16 randomised controlled trials examining the effects of exercise during or after chemotherapy and radiotherapy or after surgery compared with placebo, other treatment or standard care. Only studies that used exercise to improve or maintain physical fitness and measured health-related quality of life were included. The review included patients with mixed, breast, lymphoma, colorectal, prostate and lung cancer. Sample sizes ranged from 21 to 269 patients in the included studies. Exercise was effective for improving quality of life among cancer patients when compared to placebo, other treatment or standard care (standardised mean difference 5.6, 95% CI 3.2 to 7.9, 1,735 patients, 16 trials). Benefits of exercise were also evident for secondary outcomes (peak oxygen consumption, self-esteem, physical functioning, fatigue, length of hospital stay, number of general practitioner visits, social functioning). None of the trials included reported adverse events. There is no ideal dosage of exercise therapy for cancer patients; however exercising more frequently and in shorter workouts were associated with better outcomes in the included studies. More studies with long-term follow-ups are needed to investigate the effects of exercise on cancer recurrence and survival rates. Exercise therapy should be recommended during cancer treatment.
Gerritsen JKW, Vincent AJPE. Exercise improves quality of life in patients with cancer: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med 2016;50:796-803.
Read more on PEDro.