Return to all evidence summaries
Orthopaedics
Orthopaedics includes only fractures and intervention before or after orthopaedic surgery (eg, knee replacements, ligament repairs).
The most recently synthesised review is at the top of the list.
- The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery
- Interventions for improving mobility after hip fracture surgery in adults
- Shoulder stabilization versus immobilization for first-time anterior shoulder dislocation
The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery: a systematic review and meta-analysis of randomised controlled trials
Ankle fractures are common injuries that often require open reduction and internal fixation surgery. Post-operative rehabilitation protocols traditionally recommend late weight-bearing to avoid complications. Recently, early weight-bearing has been explored as an alternative approach to potentially accelerate recovery. This systematic review aimed to examine the effects of early weight-bearing compared to late weight-bearing on function, time to return to daily life, and safety outcomes following ankle fracture surgery.
Seven electronic databases were searched for randomized controlled trials published in English and Chinese. Eligible studies included people recovering from ankle fracture surgery of any age, with no significant co-morbidities (e.g., severe cardiovascular disease, unstable chronic conditions, or acute neurological impairments). The intervention was defined as early weight-bearing protocols, encompassing both partial and complete weight bearing, initiated within six weeks post-surgery. The comparator was late weight-bearing, starting six weeks or more post-surgery. Primary outcomes were 1) ankle function, 2) time to return to daily life and 3) complication rates. (e.g., re-fracture, wound infection). A primary timepoint post-surgery was not specified. Risk of bias was assessed using the Cochrane Risk of Bias 1.0 tool. Meta-analyses were applied using fixed effects model (if I2 < 50%) or random-effects model (if I2 > 50%). There was no assessment of the certainty of evidence.
There review included 11 trials (862 participants). Eight (73%) trials initiated early weight-bearing within six weeks post-surgery. Some trials presented an unclear or high risk of bias due to lack of concealed allocation (5 trials), blinding of participants or personnel (7 trials), and blinding of outcome assessors (4 trials).
Compared to late weight-bearing, early weight-bearing improved ankle function scores at 6 weeks (SMD 0.69, 95% CI 0.49 to 0.88, I2 = 0%), 12 weeks (SMD 0.57, 95% CI 0.22 to 0.92, I2 = 75%), 24-26 weeks post-surgery (SMD 0.52, 95% CI 0.20 to 0.85, I2 = 51%), although ankle function was not improved 1-year post-surgery (SMD 0.21, 95% CI -0.01 to 0.42). Time to return to daily life was significantly shorter in patients who received early weight-bearing (MD -2.74 weeks, 95% CI -3.46 to -2.02, I2 = 0%). Early weight-bearing did not significantly increase complications compared to late weight-bearing (RR 1.30, 95% CI: 0.85 to 1.98).
Early weight-bearing after ankle fracture surgery improves ankle function more than late weight bearing in the short term but not at 1-year post-surgery. People who receive early weight-bearing have less time away from daily life without an increase in complication rates. These findings suggest that early weight-bearing could be used instead of late weight bearing post-operative ankle fracture.
Chen B, Ye Z, Wu J, Wang G, Yu T. The effect of early weight-bearing and later weight-bearing rehabilitation interventions on outcomes after ankle fracture surgery: a systematic review and meta-analysis of randomised controlled trials. Journal of Foot and Ankle Research Published online Jun 17 2024. doi/10.1002/jfa2.12011

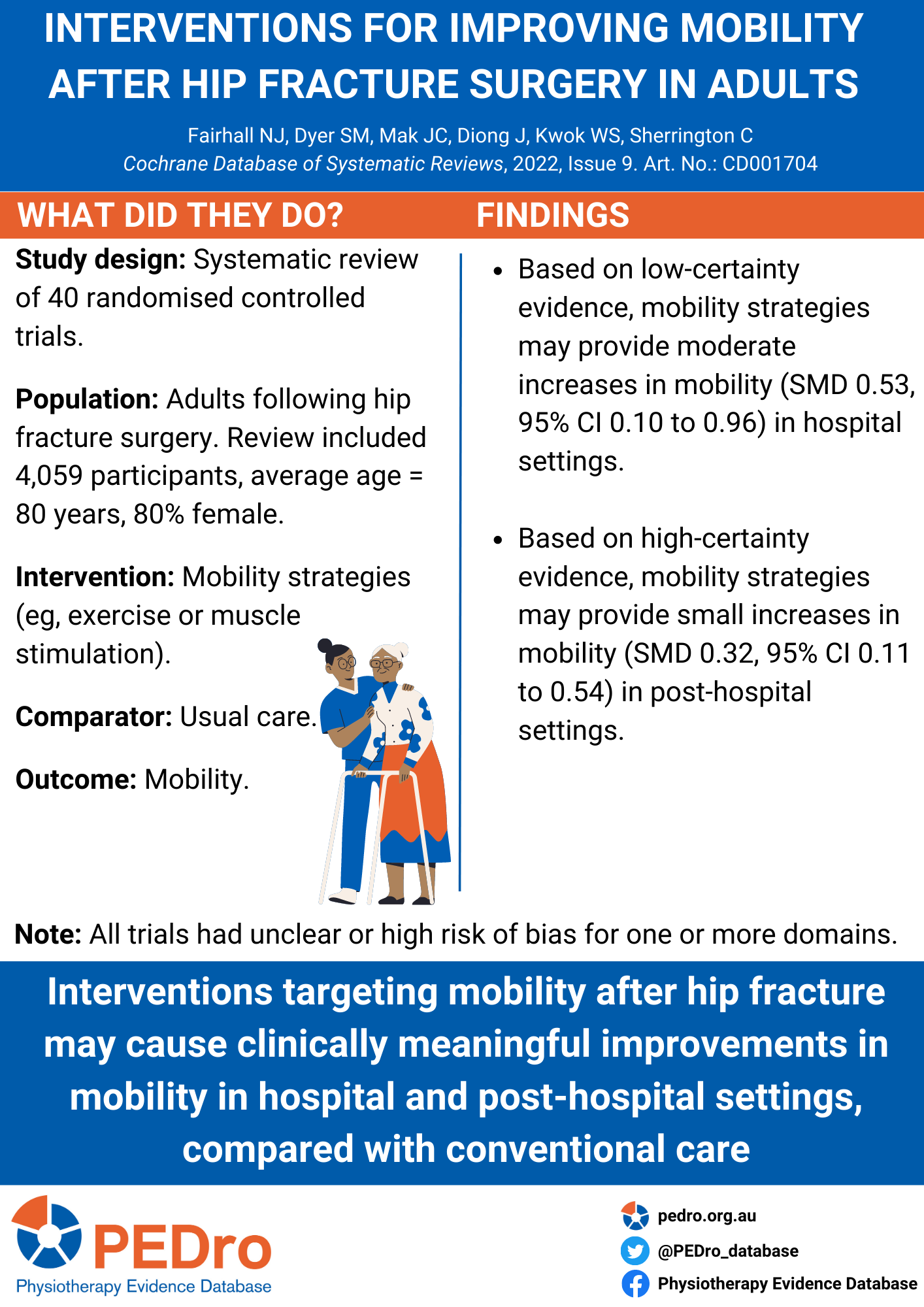
Interventions for improving mobility after hip fracture surgery in adults
Improving mobility outcomes after hip fracture is key to recovery. Mobility is the ability to move about, including standing up and walking and mobility strategies are treatments that aim to help people move better. This Cochrane systematic review aimed to evaluate the benefits and harms of interventions for improving mobility and physical functioning after hip fracture surgery in adults.
This Cochrane systematic review included randomised controlled trials or quasi-randomised controlled trials that assessed mobility strategies after hip fracture surgery. Eligible trials were identified from 8 electronic databases. Trials were included if they investigated the effect of strategies aimed to improve mobility. These could include care programmes, exercise (gait, balance, functional training, strength/resistance/endurance/flexibility training, three-dimensional exercise and general physical activity) or muscle stimulation. Interventions could be compared to usual care (both in-hospital), no intervention, sham exercise or social visits (post-hospital). Critical outcomes were mobility, walking speed, functioning, health-related quality of life, mortality, adverse effects, and return to living at pre-fracture residence.
Two reviewers identified and selected studies, extracted data, and assessed risk of bias using the Cochrane Risk of Bias 2.0 tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
The review included 40 randomised controlled trials (n = 4059 participants) from 17 countries. Patients were mostly elderly (average age 80 years) and female (80%). All trials had unclear or high risk of bias for one or more domains.
In the hospital setting, there is low certainty evidence that mobility strategies may lead to a moderate, clinically meaningful increase in mobility compared to usual care (standardised mean difference [SMD]: 0.53, 95% confidence interval [CI] 0.10 to 0.96; n = 360). Post-hospital, there is high certainty evidence that mobility strategies compared to usual care, no intervention, sham exercise or social visit led to a small, clinically meaningful increase in mobility (SMD: 0.32, 95% CI 0.11 to 0.54; n= 761). Adverse events were rarely measured by included trials so the safety of these programs in the hospital and out of hospital settings remains unknown.
Compared with conventional care, interventions that target improvement in mobility after hip fracture may improve mobility and walking speed, both in hospital and post-hospital settings. However, long term and economic outcomes have not yet been determined.
Fairhall NJ, Dyer SM, Mak JC, Diong J, Kwok WS, Sherrington C. Interventions for improving mobility after hip fracture surgery in adults. Cochrane Database Syst Rev. 2022 Sep 7;9(9):CD001704.
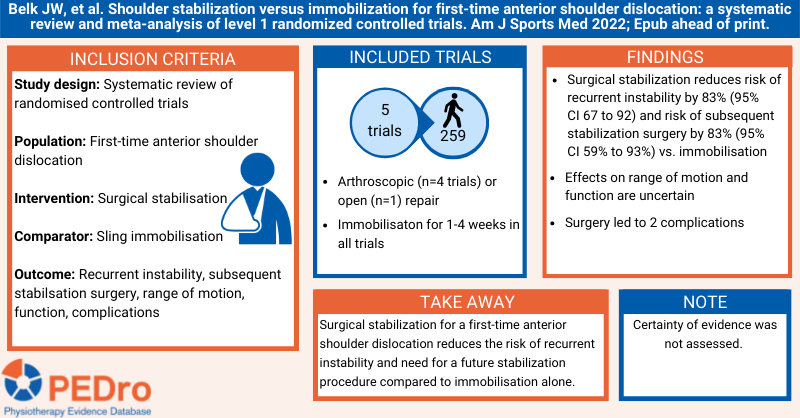
Shoulder stabilization versus immobilization for first-time anterior shoulder dislocation: a systematic review and meta-analysis of level 1 randomized controlled trials
Anterior shoulder dislocations are among the most common shoulder injuries in adolescent athletes and often occur after acute trauma. Despite multiple studies comparing rates of recurrent instability after surgical stabilisation and non-operative sling immobilisation for patients experiencing a first-time anterior shoulder dislocation, there remains uncertainty about the best treatment approach.
This systematic review aimed to estimate the effects of surgical stabilisation for people with a first-time anterior shoulder dislocation on recurrent instability, need for a future stabilisation procedure, range of motion, and function compared to sling immobilisation.
Searches were performed in seven databases (including PubMed, Embase, and Cochrane Library) to identify randomised controlled trials investigating the effects of surgical stabilisation versus sling immobilisation for the treatment of first-time anterior shoulder dislocation on rates of recurrent instability.
The outcomes were recurrent instability, subsequent stabilisation surgery, range of motion, function as assessed by the Western Ontario Shoulder Instability Index, and complications. Only outcomes reported by at least three trials were included. Two independent reviewers selected trials for inclusion. Disagreements were resolved by discussion or by arbitration from a third reviewer. Data were extracted by one reviewer and checked by a second. Trial quality was evaluated using version 1.0 of the Cochrane risk of bias tool. Meta-analysis was used to pool trials and calculate the between-group risk ratio, and the associated 95% confidence interval (CI), for recurrent instability and subsequent stabilisation surgery.
Five trials (259 participants) were included in the review. The average age of participants and percentage of males was 24 years and 87% in the operative group, and 23 years and 89% in the non-operative group. Four trials used similar arthroscopic Bankart procedures, and one used an open Bankart procedure. Participants in all trials underwent surgery between 10 and 28 days after anterior shoulder dislocation and were placed in an internally rotated sling immobiliser for 1-4 weeks post-operatively. The non-operative approach in 4 trials involved placing participants in an internal rotation sling for 1-4 weeks. In 1 trial, participants were placed in an external rotation and abduction immobiliser for 3 weeks. Physiotherapy protocols were identical between the operative and non-operative groups across trials and involved minimal active or passive movement through the immobilisation phase (about 3 weeks), active external rotation and abduction until 6 weeks, unrestricted range of motion after 6-12 weeks, and resistance exercises thereafter. All trials were at high risk of bias due to being unable to blind participants (performance bias) and therapists and/or outcome assessors (detection bias).
Surgical stabilisation reduced the risk of recurrent instability by 83% (95% CI 67% to 92%) and the risk of subsequent stabilisation surgery by 83% (95% CI 59% to 93%) compared to sling immobilisation. Findings were the same when only including trials in which participants in the non-operative group were immobilised in internal rotation. All 3 trials that assessed range of motion found no difference between surgical stabilisation and sling immobilisation. Of the 3 trials that assessed Western Ontario Shoulder Instability Index scores, 1 found higher scores in the operative group and 2 found no difference. Two complications were reported in the operative group and none in the non-operative group.
Surgical stabilisation for a first-time anterior shoulder dislocation reduces the risk of recurrent instability and need for a future stabilisation procedure compared to non-operative management involving sling immobilisation. It is uncertain whether surgical stabilisation is superior to non-operative management for improving shoulder function and range of motion.
Belk JW, et al. Shoulder stabilization versus immobilization for first-time anterior shoulder dislocation: a systematic review and meta-analysis of level 1 randomized controlled trials. Am J Sports Med 2022 Feb 11:Epub ahead of print.