Return to all evidence summaries
Other
The most recently synthesised review is at the top of the list.
- Do digital interventions increase adherence to home exercise rehabilitation?
- Effects of gamified smartphone applications on physical activity
- Dose-dependent effect of supervised aerobic exercise on hba1c in patients with type 2 diabetes
- Behaviour change interventions to increase physical activity in hospitalised patients
- Aerobic exercise alleviates depressive symptoms in patients with a major non-communicable chronic disease
- Association of efficacy of resistance exercise training with depressive symptoms
Do digital interventions increase adherence to home exercise rehabilitation?
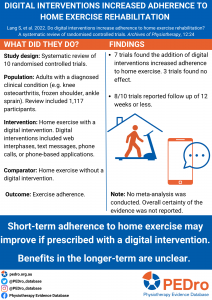
This systematic review aimed to estimate the effects of an additional digital intervention compared to no digital intervention on adherence to a prescribed home exercise program in people with a diagnosed clinical condition.
This was a systematic review of randomised controlled trails (RCTs). RCTs were included if their primary outcome was exercise adherence and participants in the trial received a prescription of home exercises for a specific clinical condition either with (intervention group) or without (control group) an additional digital intervention. Digital interventions included any intervention that was delivered through a communication platform or electronic device. One reviewer screened titles and two independent reviewers screened abstracts and full texts for inclusion. Risk of bias was assessed by two independent reviewers using the Cochrane Risk of Bias tool.
10 RCTs were included in the review involving 1,117 participants. 565 participants were randomised to the intervention group and 552 to the control group. Trial size varied from 20 to 152 participants and mean age ranged from 37.5 to 79.5 years. Trials were conducted in Australia, Europe, Asia, the Middle East, and North America. Clinical conditions included knee osteoarthritis, frozen shoulder, ankle sprain, flexor digitorium profundus repair, mixed musculoskeletal conditions, and stroke. Digital interventions included web interphases, text messages, phone calls, and phone-based applications. Follow-up adherence ranged from 2-weeks to 24-months, with a median of 17.9 weeks.
7 RCTs found that the addition of a digital intervention increased adherence to the home exercise program. The remaining 3 RCTs found no group differences. All studies reporting short-term follow-up (<6 weeks; 4 RCTs) and half of the studies reporting medium-term follow-up (8-12 weeks; 2 out of 4 RCTs) or long-term follow-up (24-months; 1 out of 2 RCTs) found positive effects of digital interventions on home exercise program adherence. Overall risk of bias of included studies was moderate to high.
Short-term adherence to home exercise programs may improve if prescribed with an additional digital intervention. Benefits in the longer-term are unclear.
Lang, S, McLelland, C, MacDonald, D & Hamilton, D 2022, “Do digital interventions increase adherence to home exercise rehabilitation? A systematic review of randomised controlled trials” Archives of Physiotherapy, 12:24
Effects of gamified smartphone applications on physical activity
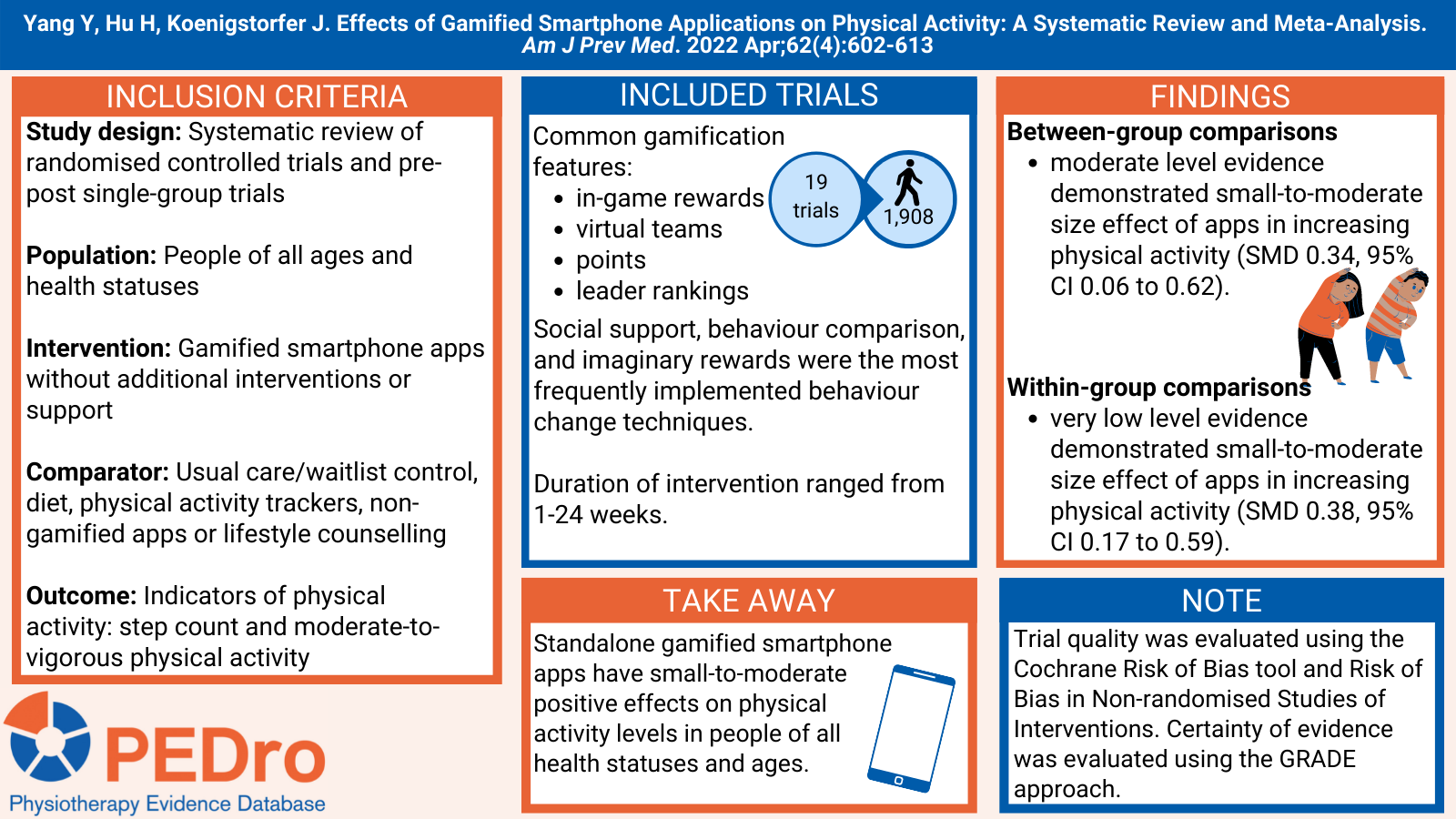
Many people do not meet the recommended levels of physical activity. Strategies are needed to improve motivation for increasing and sustaining physical activity levels. Gamification of smartphone apps involves using game design elements including storytelling, avatars, collection of points and mastery of challenges which aim to increase intrinsic motivation of behaviours, such as physical activity. This systematic review aimed to estimate the effects of standalone gamified smartphone app-delivered interventions compared to a control group (for randomised controlled trials (RCTs)) or pre-post measures (for single-group studies) on physical activity in people of any age and any health status.
Guided by a registered protocol, 5 databases (including Web of Science, Scopus and PubMed) were used to search for RCTs and pre-post single-group studies published in English between 2008 (when literature on gamification was first published) to August 31st 2021. Eligible studies included participants of any age and health status. The interventions were gamified smartphone apps for physical activity that did not involve additional interventions or support. For RCTs, comparator groups varied and included usual care/waitlist control, diet, physical activity trackers (e.g., Calorific, Fitbit), apps (e.g., WeChat Sports) or lifestyle counselling. Indicators of physical activity was the outcome of interest (e.g., moderate-to-vigorous physical activity, step counts). Studies involving exergames, video games or serious games were excluded.
Title, abstract, and full-text screening for eligibility, and data extraction were performed by two authors independently, with disagreements resolved by a third author. The Cochrane Risk of Bias (RoB-2) and the Risk of Bias in Non-randomised Studies of Interventions (ROBINS-I) tools were used to assess the methodological quality of RCTs and single-group studies, respectively. A meta-analysis pooled the trials using standardised mean differences (SMD, based on Hedge’s g) to summarise and compare between-group (RCTs only) and within-group differences (pre-post measures of all intervention groups). A meta-regression was performed for sex (% female) and intervention duration. Subgroup analyses explored the effect of study population, age group, study design, physical activity measures (subjective/objective) and type of comparator on indicators of physical activity. Sensitivity analyses were conducted to investigate the effect of heterogeneity and risk of bias on the meta-analysis. Evidence quality was evaluated using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach.
Nineteen studies, 17 RCTs and 2 pre-post single-group studies, involving 1,908 participants were included in the systematic review. Fifteen studies included adults and 17 studies were based on healthy cohorts. Commonly used gamification features were in-game rewards, virtual teams, points/scores and leader boards/rankings. Social support, behaviour comparison, and imaginary rewards were the most frequently implemented behaviour change techniques. The intervention duration was a median of seven weeks (range 1-24 weeks). Thirteen studies measured physical activity objectively, 2 used questionnaires and 4 used combined methods. 15 studies were rated as having ‘some concerns’ in terms of study quality which was due to deviations from the intended interventions and outcome measurement.
Sixteen studies were included in the meta-analysis. In between-group comparisons, moderate level evidence demonstrated small-to-moderate size effects supporting the use of apps to increase physical activity (n=12 apps, SMD 0.34; 95% CI 0.06 to 0.62, I2=72%). In within-group comparisons, very low level evidence demonstrated small-to-moderate size effects supporting the use of apps to increase physical activity (n=18 apps, SMD 0.38; 95% CI 0.17 to 0.59, I2=74%). Only in the between-group comparisons, both increased intervention duration (n=12 apps, SMD 0.05; 95% CI 0.01, 0.08) and being male (n=12, SMD -0.01 [female]; 95% CI -0.02 to -0.00) had a small but significant modifying effect on the intervention. Between-group subgroup analyses showed larger effects for patients (SMD 1.63; 95% CI -0.5, 3.31) compared to healthy populations (SMD 0.18; 95% CI 0.0 to 0.35). In within-group subgroup analyses, there was a moderate-to-large effect of apps on step counts (n=8, SMD 0.69; 95% CI 0.24 to 1.15), but small-to-moderate effect on moderate-to-vigorous physical activity (n=10, SMD 0.18; 95% CI 0.05 to 0.31).
Very low to moderate level evidence suggests that standalone gamified smartphone apps have small-to-moderate positive effects on physical activity levels in people of all health statuses and ages, compared to usual care/waitlist control, diet, physical activity trackers, non-gamified apps or lifestyle counselling. Findings support the use of digital health technologies to improve physical activity. Future research is required to determine which intervention features are effective in maintaining behaviour change.
Yang Y, Hu H, Koenigstorfer J. Effects of Gamified Smartphone Applications on Physical Activity: A Systematic Review and Meta-Analysis. Am J Prev Med. 2022 Apr;62(4):602-613. doi: 10.1016/j.amepre.2021.10.005. Epub 2021 Dec 7. PMID: 34893387.
Dose-dependent effect of supervised aerobic exercise on hba1c in patients with type 2 diabetes
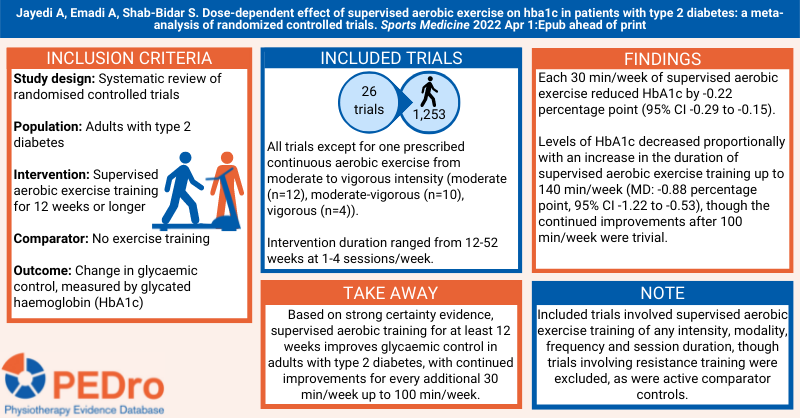
Type 2 diabetes is a global public health concern, with increasing incidence and financial burden. Improving glycaemic control (measured by glycated haemoglobin, HbA1c) reduces risks of microvascular complications and cardiovascular disease events. Previous systematic reviews indicated aerobic exercise improves glycaemic control, but the optimum dose of exercise was unknown. This systematic review aimed to estimate the dose-dependent effects of supervised aerobic exercise training of 12 weeks or longer compared to no intervention or usual activity (control group) on levels of HbA1c in people with type 2 diabetes.
Guided by a prospectively registered protocol, sensitive searches of three databases (including PubMed, Scopus and Web of Science) and citation tracking were performed to identify randomised controlled trials evaluating supervised aerobic training. The participants were people with type 2 diabetes aged 18 years and older. The intervention was supervised aerobic exercise training of any intensity, modality, frequency and session duration in a program for 12 weeks or longer. Trials were excluded that implemented combined aerobic and resistance exercise training or had an active control group (e.g. resistance training). The primary outcome was change in HbA1c (%). In addition to reporting HbA1c, included trials needed to report the duration and intensity of the aerobic training for the intervention group. Two reviewers independently selected trials, extracted data and evaluated trial quality. Disagreements were resolved through discussion or arbitration by a third reviewer. Trial quality was assessed using the Cochrane risk of bias tool. Certainty of the evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Dose-response meta-analysis was used to calculate the mean between-group difference and 95% confidence interval (CI) to illustrate the dose-dependent effect of duration (min/week) of supervised aerobic exercise on HbA1c. Pre-defined subgroup analyses were based on baseline weight and health status, exercise modality and intensity, intervention duration, presence of dietary co-intervention, and risk of bias assessment.
Twenty-six trials (1,253 participants) published between 1994 and 2020 were included in this review. The trials were conducted in North and South America, Europe, Africa, Asia and Oceania. Nineteen trials included men and women, five included women only and two included men only. Participants were a mix of weight ranges (normal weight, overweight and obese) and varied incidence of comorbidities or diabetic complications. Intervention duration ranged from 12 to 52 weeks. Frequency of supervised aerobic exercise training was 1-4 sessions/week. Twelve trials implemented a moderate intensity aerobic exercise training program, 10 trials a moderate-to-vigorous intensity program, and four trials a vigorous intensity program. All trials implemented continuous aerobic exercise, except for one study which implemented high-intensity interval training. Fourteen trials implemented a non-progressive aerobic exercise program and the other 12 trials progressed training in terms of frequency, intensity or duration.
Each 30 min/week supervised aerobic exercise reduced HbA1c by -0.22 percentage point (95% CI -0.29 to -0.15; 26 trials; 1253 participants; strong certainty). The subgroup analyses produced similar results for the baseline participant characteristics, program design and risk of bias. Levels of HbA1c decreased proportionally with an increase in the duration of supervised aerobic exercise training up to 140 min/week (MD: -0.88 percentage point, 95% CI -1.22 to -0.53), though the continued improvements after 100 min/week were trivial.
Every 30 min/week supervised moderate-to-vigorous intensity aerobic exercise training reduced HbA1c by 0.22 percentage point. The greatest reduction was seen at 140 min/week, however durations above 100 min/week do not further decrease HbA1c. The certainty of the evidence was rated strong based on the GRADE approach.
Jayedi A, Emadi A, Shab-Bidar S. Dose-dependent effect of supervised aerobic exercise on hba1c in patients with type 2 diabetes: a meta-analysis of randomized controlled trials. Sports Medicine 2022 Apr 1:Epub ahead of print https://doi.org/10.1007/s40279-022-01673-4
Behaviour change interventions to increase physical activity in hospitalised patients
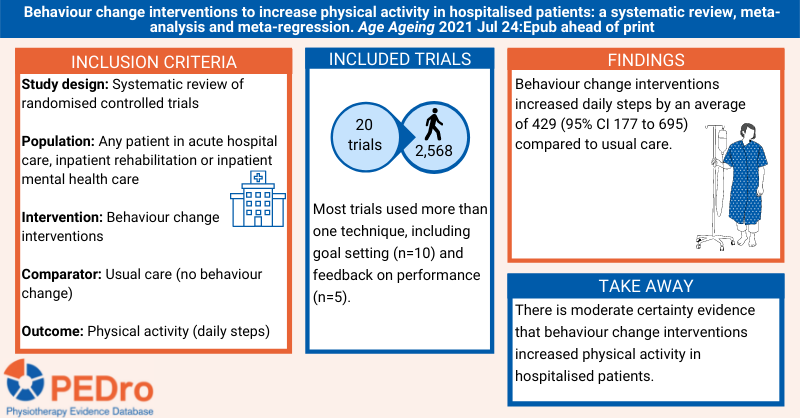
Admission to hospital for treatment of many health conditions is associated with impaired mobility and a period of bed rest that can lead to reduced physical activity. These low levels of physical activity observed during hospital admission predispose patients to the secondary consequences of inactivity, particularly deconditioning and increased risk of adverse events and mortality. Behaviour change interventions (eg, goal setting, self-monitoring, providing feedback on performance, goal review) are used to increase physical activity. Previous reviews have evaluated the impact of behaviour change interventions on physical activity levels in community or outpatient settings and in people with chronic conditions. This systematic review aimed to estimate the effects of behaviour change interventions compared to usual care on physical activity levels in the inpatient setting. A secondary objective was to explore the association between specific behaviour change techniques and increased physical activity in hospitalised patients.
Guided by a prospectively registered protocol, sensitive searches in 6 databases (including Medline and PEDro) and citation tracking were performed to identify randomised controlled trials evaluating behaviour change interventions applied in inpatient settings. The patients were people of any age who were hospitalised for any physical or mental health condition, including acute hospital care, inpatient rehabilitation, and inpatient mental health care. Behaviour change interventions included those described in the 40-item taxonomy of behaviour change techniques. The comparator was usual care (ie, hospitalised patients who did not receive the behaviour change interventions). The primary outcome was any objective measure of physical activity assessed during the admission (eg, daily steps, activity counts). Two reviewers independently selected trials for inclusion, extracted data, classified the behaviour change techniques used in the intervention, and evaluated trial quality (Cochrane risk of bias 2 tool). Any disagreements were resolved by discussion or arbitration by a third reviewer. Certainty of evidence was evaluated using the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) approach. Meta-analysis was used to pool the trials, with the between-group differences reported as standardised mean differences or weighted mean differences and their 95% confidence intervals (CI). One subgroup analysis was planned for setting: acute hospital care vs. inpatient rehabilitation. Meta-regression was used to explore associations between the behaviour change techniques used in more than three trials and the treatment effects.
20 trials (2,568 participants) were included in the review. The average age of participants was 67 years and 56% were women. The most common diagnosis was stroke (4 trials). 14 trials were conducted in acute hospital care (10 surgical, 3 medical, 1 mixed surgical/medical) and 6 in inpatient rehabilitation. 23 behaviour change techniques were used across the included trials, with most trials using more than one technique. The techniques used by more than three trials were goal setting (10 trials), feedback on performance (8 trials), reviewing behavioural goals (4 trials) and instructing on how to perform a behaviour (4 trials). The interventions were commonly applied by physiotherapists in at least daily, face-to-face sessions with individual patients.
Different outcome measures were used to quantify physical activity, so the standardised mean difference was calculated. On average, participants receiving behaviour change interventions had higher physical activity than those receiving usual care (standardised mean difference 0.34; 95% CI 0.14 to 0.55; 18 trials; 1,730 participants; moderate certainty). This translates to a mean of 429 more steps/day (95% CI 177 to 695), the outcome measure used in the review when physical activity was measured with more than one method, for behaviour change intervention compared to usual care. [Note: the weighted average baseline standard deviation across all groups from the three included trials reporting physical activity in steps/day (https://dx.doi.org/10.1177/0269215518755841, https://dx.doi.org/10.1016/j.jphys.2019.08.006, https://dx.doi.org/10.1177/0269215519901153) and guidance from the Cochrane Handbook v6.1 were used to calculate this estimate].
The subgroup analysis suggests that larger effects were observed in acute hospital care (standardised mean difference 0.46; 95% CI 0.16 to 0.75; 12 trials; 1,039 participants) than in inpatient rehabilitation (standardised mean difference 0.16; 95% CI -0.08 to 0.40; 6 trials; 691 participants). Meta-regression found that the behaviour change technique of goal setting (standardised mean difference 0.29; 95% CI 0.05 to 0.53; 10 trials) was independently associated with increasing physical activity compared to usual care, but feedback (standardised mean difference 0.25; 95% CI -0.02 to 0.53; 8 trials), reviewing of behavioural goals (standardised mean difference 0.24; 95% CI -0.12 to 0.61; 4 trials), and providing instruction on how to perform a behaviour (standardised mean difference 0.24; 95% CI -0.12 to 0.59; 4 trials) were not.
Targeted behaviour change interventions were associated with increases in physical activity in hospitalised patients compared to usual care, with the behaviour change technique of goal setting being particularly important.
Taylor NF, et al. Behaviour change interventions to increase physical activity in hospitalised patients: a systematic review, meta-analysis and meta-regression. Age Ageing 2021 Jul 24:Epub ahead of print
Aerobic exercise alleviates depressive symptoms in patients with a major non-communicable chronic disease
People with non-communicable chronic health conditions such as cardiovascular disease, cancer, respiratory disease and type 2 diabetes have higher rates of symptoms of depression than the general population. Symptoms of depression are also an adverse prognostic factor for these conditions. Aerobic exercise is accepted as an effective treatment option for depression in people without comorbid chronic disease. This systematic review aimed to estimate the effects of aerobic exercise compared to usual care on symptoms of depression in people with chronic diseases.
Sensitive searches of three databases identified (non-)randomised controlled trials that recruited adults with cardiovascular disease, cancer, respiratory disease or type 2 diabetes. Trials had to compare an aerobic exercise intervention (delivered at least twice per week, achieving at least moderate intensity exercise, for a minimum of 4 weeks) to usual care. Trials where usual care involved any type of exercise were excluded. The outcome was depression assessed by clinical assessment or symptoms of depression measured using a validated questionnaire. Two independent reviewers selected trials and extracted the data. Trial quality was evaluated with the Downs and Black checklist and certainty of the evidence with the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) tool. Meta-analyses were reported as standardised mean difference (SMD) and 95% confidence interval (CI). Five subgroup analyses were prespecified and estimated via meta-regression: (1) type of condition; (2) frequency of exercise < =3 vs. >3 sessions/week; (3) duration of sessions < =30 vs. >30 minutes; (4) length of program <12 vs. >=12 weeks.
30 randomised controlled trials and 2 non-randomised trials (4,111 participants) were included in the review, 24 of which reported data suitable for meta-analysis. Interventions were delivered 2 to 5 sessions/week for 20 to 80 minutes/session for 4 to 24 weeks. Eleven studies included people with cardiovascular disease, 10 with cancer, 2 with respiratory disease and 1 with diabetes.
There was low certainty evidence that exercise improved symptoms of depression in people with chronic conditions (SMD 0.5, 95% CI 0.25 to 0.76, 24 trials) compared to usual care. There was moderate certainty evidence that aerobic exercise improved symptoms of depression in cardiovascular disease (SMD 0.67, 95% CI 0.35 to 0.99, 11 trials), and low certainty in cancer (SMD 0.22, 95% CI 0.07 to 0.37, 10 trials). There was low certainty of no effect in respiratory disease (SMD 0.98, 95% CI -0.01 to 1.96, 2 trials) and diabetes (SMD 0.11, 95% CI -0.43 to 0.65, 1 trial). Meta-regression did not show that session frequency, session duration or program length influenced effect size.
Aerobic exercise has potentially clinically important effects on symptoms of depression in people with chronic non-communicable diseases. Certainty of evidence is strongest in people with cardiovascular disease. The exercise programs investigated targeted the health effects of the chronic conditions and were not specifically designed for symptoms of depression per se. It is also worth noting that this systematic review did not aim to assess the effect of exercise in people with clinical diagnosis of major depressive disorder.
Beland M, et al. Aerobic exercise alleviates depressive symptoms in patients with a major non-communicable chronic disease: a systematic review and meta-analysis. Brit J Sports Med 2020;54:272-8
Association of efficacy of resistance exercise training with depressive symptoms
This recent systematic review evaluated the effect of resistance exercise training in people with depressive symptoms. The primary outcome was depressive symptoms measured with a validated scale. Four moderator variables were selected a priori and their contribution to the variation in the effect size was tested through meta-regression: total volume of prescribed resistance exercise training, participant’s health status, whether or not allocation was concealed and/or assessment of outcome measures was blinded, and whether or not the resistance exercise training intervention resulted in a significant improvement in strength. The review included 54 comparisons from 33 randomised controlled trials (1,877 participants). 25 trials evaluated participants with physical or mental illness. Health care professionals fully supervised the strength training in 25 comparisons, while seven were a combination of supervised and unsupervised sessions and one was unsupervised. The mean duration of the resistance exercise training was 16 weeks (range 6 to 52 weeks). The frequency of training sessions ranged from 2 to 7 days per week. The pooled effect size (Hedges d) was 0.66 (95% confidence interval 0.48 to 0.83). Meta-regression revealed that among the moderator variables, only concealed allocation and/or blinding of outcome assessment influenced the effect size. A comparison between resistance training and aerobic training revealed that the two interventions had similar effects. This review has shown that resistance exercise training was associated with a significant reduction in depressive symptoms regardless of the participant’s characteristics (i.e. age, sex and health status) or features of training (i.e. program duration, session duration, intensity, frequency, or total prescribed volume).
Listen to Norman Swan interview Brett Gordon (a doctoral student from the University of Limerick who is the lead author of this review) for ABC Radio National’s Health Report.
Gordon BR et al. Association of efficacy of resistance exercise training with depressive symptoms: meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiatry 2018;75(6):566-76