Return to all evidence summaries
Paediatrics
Paediatrics includes papers where the average age of the study sample is under 16, and papers on conditions which commonly affect children (eg, cystic fibrosis).
The most recently synthesised review is at the top of the list.
- Aquatic Compared With Land-Based Exercises on Gross Motor Function of Children/Adolescents With Cerebral Palsy
- Physiotherapeutic scoliosis-specific exercise for the treatment of adolescent idiopathic scoliosis
- Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer
- Physical activity and exercise training in cystic fibrosis
- Psychosocial Interventions for the Treatment of Functional Abdominal Pain Disorders in Children: A Systematic Review and Meta-analysis
- Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes
- Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions
- The Effectiveness of Physical Therapy Interventions for Athletes Post-Concussion
Aquatic Compared With Land-Based Exercises on Gross Motor Function of Children/Adolescents With Cerebral Palsy
Cerebral palsy (CP) is a common childhood disability characterised by motor impairments that affect mobility and functional skills. Rehabilitation programs aim to improve fitness, mobility, and participation through interventions such as fitness, strength and mobility training and task-specific exercises. Aquatic-based exercises, which utilise water’s buoyancy and thermal effects, may reduce joint stress, promote trunk control and muscle activation and enhance motivation. Previous systematic reviews have evaluated aquatic therapy benefits but have not compared aquatic- and land-based exercise effects on gross motor function in this population. The aim of this systematic review and meta-analysis was to compare the effects of aquatic-based versus land-based exercises on gross motor function in children and adolescents with CP.
The review followed PRISMA guidelines and was prospectively registered on PROSPERO (CRD42020194121). Searches across eight databases (PubMed, Cochrane Library, Scopus, Web of Science, EMBASE, SciELO Citation Index, LILACS and CINAHL), citation tracking and clinical trial registries of randomised controlled trials (RCTs) involving children aged 2–18 years with CP. Eligible interventions were structured aquatic-based exercises compared with land-based programs. Outcomes were measured using standardised tools such as the Gross Motor Function Measure (GMFM). Data extraction was performed independently by three reviewers. Risk of bias was assessed using the PEDro scale, and evidence quality was rated using GRADE. Meta-analyses were conducted using fixed-effects models. Effect sizes were reported standardized mean differences (SMD) with 95% confidence intervals. Subgroup analyses evaluated the effects of different aquatic exercise types (aquatic physical therapy, Halliwick method, swimming exercises, gait training and water exercises).
Fifteen RCTs published between 2007 and 2023 were included, involving 369 participants aged 2–18 years. Most participants were ambulatory and classified as Gross Motor Function Classification System levels I–III with spastic hemiparetic or diparetic CP. Interventions varied: five studies used aquatic physical therapy, five applied the Halliwick method, three focused on swimming, one on gait training in water, and one on aqua-plyometric exercises. Land-based programs included neurodevelopmental treatment approaches, functional activities and combinations of stretching, strengthening, gait and balance training. Most interventions lasted 10–12 weeks, with session durations 30–60 minutes, twice weekly. Risk of bias was high overall, frequently due to lack of concealed allocation, incomplete follow-up and lack of intention-to-treat analysis; only six studies were rated as good quality.
Meta-analysis of 13 trials (n=253) showed very low-quality evidence that aquatic-based exercises improved gross motor function compared to land-based exercises (SMD 0.45, 95% CI 0.24 to 0.66, p<0.001), indicating a small effect size. Subgroup analysis revealed low quality evidence of benefit for aquatic physical therapy (SMD 0.47, 95% CI 0.05 to 0.89, 4 trials, n=93, p=0.03). No significant differences for Halliwick method (SMD 0.33, 95% CI -0.01 to0.67, 4 trials, n=138, p=0.06, low quality evidence) or swimming exercises (SMD 0.47, 95% CI -0.09 to 1.03, 3 trials, n=52, p=0.10). Overall, heterogeneity was low (I²=0 to 5%), but methodological limitations and small sample sizes reduced confidence in findings. Few studies reported on adverse events and they were not assessed in the review.
Aquatic-based exercises, particularly aquatic physical therapy, may offer small improvements in gross motor function compared to land-based programs for children and adolescents with CP. However, evidence quality was low due to high risk of bias, small sample sizes, and intervention heterogeneity. Aquatic therapy could serve as an adjunct or alternative to land-based therapy, but decisions should consider accessibility, cost, and patient preference. Future research should involve well-designed trials with adequate sample sizes and standardised protocols.
Pauluka E, Ceolin LS, Fontanela LC, Dos Santos AN. Aquatic Compared With Land-Based Exercises on Gross Motor Function of Children/Adolescents With Cerebral Palsy: A Systematic Review With Meta-Analysis. Child Care Health Dev. 2025 Jan;51(1):e70023. doi: 10.1111/cch.70023.

Physiotherapeutic scoliosis-specific exercise for the treatment of adolescent idiopathic scoliosis
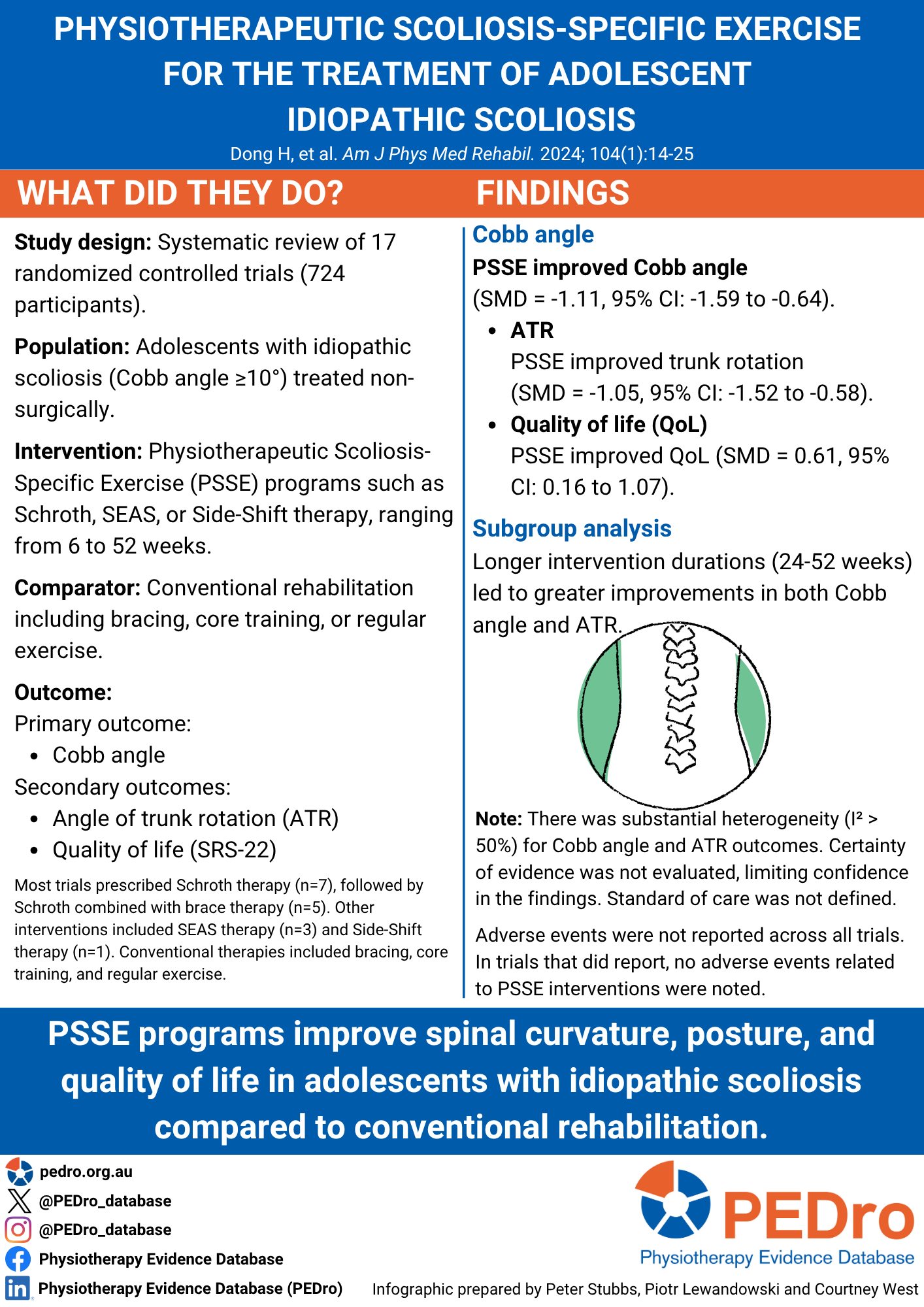
Idiopathic scoliosis is a S-shaped curvature of the spine, defined as having a Cobb angle of 10 degrees or more. Without treatment, progressive spinal deformities can limit cardiorespiratory function, coordination, balance, and quality of life. Non-surgical approaches to adolescent idiopathic scoliosis include conventional rehabilitation (eg. braces, and standard care) or physiotherapy scoliosis-specific exercise (PSSE) . PSSE includes Schroth therapy, Scientific Exercise Approach to Scoliosis (SEAS) therapy, and Side-Shift Therapy. This systematic review aimed to determine the efficacy of PSEE in improving the Cobb angle in adolescents with idiopathic scoliosis compared to conventional rehabilitation.
Eight databases were searched for randomised controlled trials (RCTs) published in English and Chinese. Studies with poor methodological quality or incomplete data were excluded. Eligible studies included adolescents diagnosed with idiopathic scoliosis according to the 2016 SOSORT guidelines. The intervention was any PSSE-based rehabilitation such as Schroth, SEAS, BSPTS, Dobomed, Side Shift, FITS, and Lyon. The comparator was any conventional rehabilitation including brace therapy, core training, regular exercise, proprioceptive neuromuscular facilitation, or standard care. The Cobb angle was the primary outcome of interest with secondary outcomes include angle of trunk rotation (ATR) and quality of life, as measured by the Scoliosis Research Society – 22 item questionnaire (SRS-22). Study selection and assessment of methodological quality, using the Cochrane Risk of Bias Tool, were performed by two authors. Evidence certainty was not assessed. A meta-analysis pooled the trials, with forest plots used to summarise and compare trials. A random effects model was used if significant heterogeneity was found (I2>50%).
Seventeen trials, involving 724 participants, were included. Trials investigated five types of PSSE therapies: Schroth combined with SEAS therapy (n=1), Schroth combined with brace therapy (5 trials), Schroth alone (7 trials), SEAS alone (3 trials), or Side-Shift therapy (1 trial). Interventions ranged from 30-90 minutes per session, 1-7 days a week for 6-52 weeks. Conventional therapies included bracing (7 trials), standard care (6 trials), core training (2 trials), PNF (1 trial), or regular training (1 trial). Unclear or high risk of bias was due to lack of concealed allocation (11 trials); blinding of participants or personnel (11 trials); blinding of outcome assessors (9 trials); and selective reporting bias (9 trials ). The frequency of adverse events was not reported in the systematic review.
Compared to conventional rehabilitation, PSSE therapies improved Cobb angle (SMD = -1.11, 95% CI: -1.59 to -0.64, n = 724, 17 trials, I2= 89%); ATR (SMD = -1.05, 95% CI: -1.52 to -0.58, n = 622, 13 trials, I2= 85%); quality of life (SMD = 0.61, 95% CI: 0.16 to 1.07, n = 333, 7 trials, I2= 74%). Amount of improvement in Cobb angle differed by intervention duration: 6-24 weeks (SMD = -0.77, 95% CI: -1.11 to -0.43, n = 150, 5 trials, I2= 1%); 24-52 weeks (SMD = -1.04, 95% CI: -1.29 to -0.79, n = 287, 6 trials, I2= 7%). Amount of improvement in ATR also differed by intervention duration: 6-24 weeks (SMD = -0.37, 95% CI: -0.7 to -0.04, n = 150, 5 trials, I2= 0%); 24-52 weeks (SMD = -1.53, 95% CI: -2.22 to -0.84, n = 472, 8 trials, I2= 89%).
PSSE therapies may improve body posture, trunk rotation, and quality of life in adolescents with idiopathic scoliosis compared to conventional rehabilitation.
Dong H, You M, Li Y, Wang B, Huang H. Physiotherapeutic Scoliosis-Specific Exercise for the treatment of adolescent idiopathic scoliosis: A systematic review and network meta-analysis. Am J Phys Med Rehabil. Published online May 10, 2024.
Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer
Individuals affected by childhood cancer may experience long-term cognitive impairments. Although exercise has been recommended for other cancer-related symptoms, the effect of physical activity on cognitive functioning in those affected by childhood cancer remains unknown. This systematic review aimed to estimate the effects of physical activity interventions compared to no intervention or usual care on cognitive function in people affected by childhood cancer.
Seven electronic databases were searched for randomised (RCTs) and quasi-randomised controlled trials, and non-randomised studies of interventions (NRSIs). There were no language or date restrictions. Eligible studies included individuals diagnosed with cancer at age 0-19 who received or are receiving cancer treatment. The intervention could be any frequency, intensity, volume, duration, or type of exercise or physical activity and delivered in any setting (e.g., gym). Control participants either had no treatment or usual care. The primary outcome of interest was performance on any standardised and objective academic or neuropsychological test of cognitive function. Outcomes related to cognitive function were categorised into 6 domains: complex attention, executive function, learning and memory, language, perceptual-motor function, and social cognition. Two independent reviewers screened for eligible studies, data extraction, assessment of risk of bias and certainty of evidence. Risk of bias was assessed using the Cochrane Risk of Bias Tool 2 for randomised and quasi-randomised controlled trials. Certainty of evidence was assessed for each outcome using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach. A meta-analysis pooled all trials using a random-effects model to estimate the standardised mean difference (Hedges’ g) between the intervention and control conditions at the end of the intervention period. A composite score was calculated for each study to determine the overall intervention effect on general cognitive performance, which was used in the meta-analysis of the primary outcome.
Twenty-two studies were included in the review (n = 1,277). The median age at recruitment was 12 years (IQR 11-14), and the median time since treatment completion was 2.5 years (IQR -1.1-3.0). Interventions included aerobic, strengthening, and/or coordination-based exercises, with a median period of 12 weeks (IQR 10.24). Sessions lasted a median duration of 45 minutes (IQR 40-60) across a median of 3 days/week (IQR 2.5-5.0). Adverse events were reported in two studies, of which nine events were noted (minor wrist cut, muscle strain, nausea, vomiting, drop in systolic blood pressure, dizziness, and nosebleed).
Five randomised controlled trials (n = 245) were included in the meta-analysis of the primary outcome. No RCT in the primary outcome meta-analysis was considered high risk of bias. There was moderate certainty evidence that physical activity resulted in small-to-moderate improvements in objective tests of cognitive function compared with control (SMD 0.40, 95% CI 0.07 to 0.73).
Physical activity and exercise interventions improve cognitive function in people who had childhood cancer. Future research should explore the optimal frequency, intensity, volume, duration, and type of physical intervention across different patient characteristics (e.g., type of cancer) for improving cognitive function.
Bernal JDK, Recchia F, Yu DJ, et al. Physical activity and exercise for cancer-related cognitive impairment among individuals affected by childhood cancer: a systematic review and meta-analysis. Lancet Child Adolesc Health. 2023;7(1):47-58.
Physical activity and exercise training in cystic fibrosis
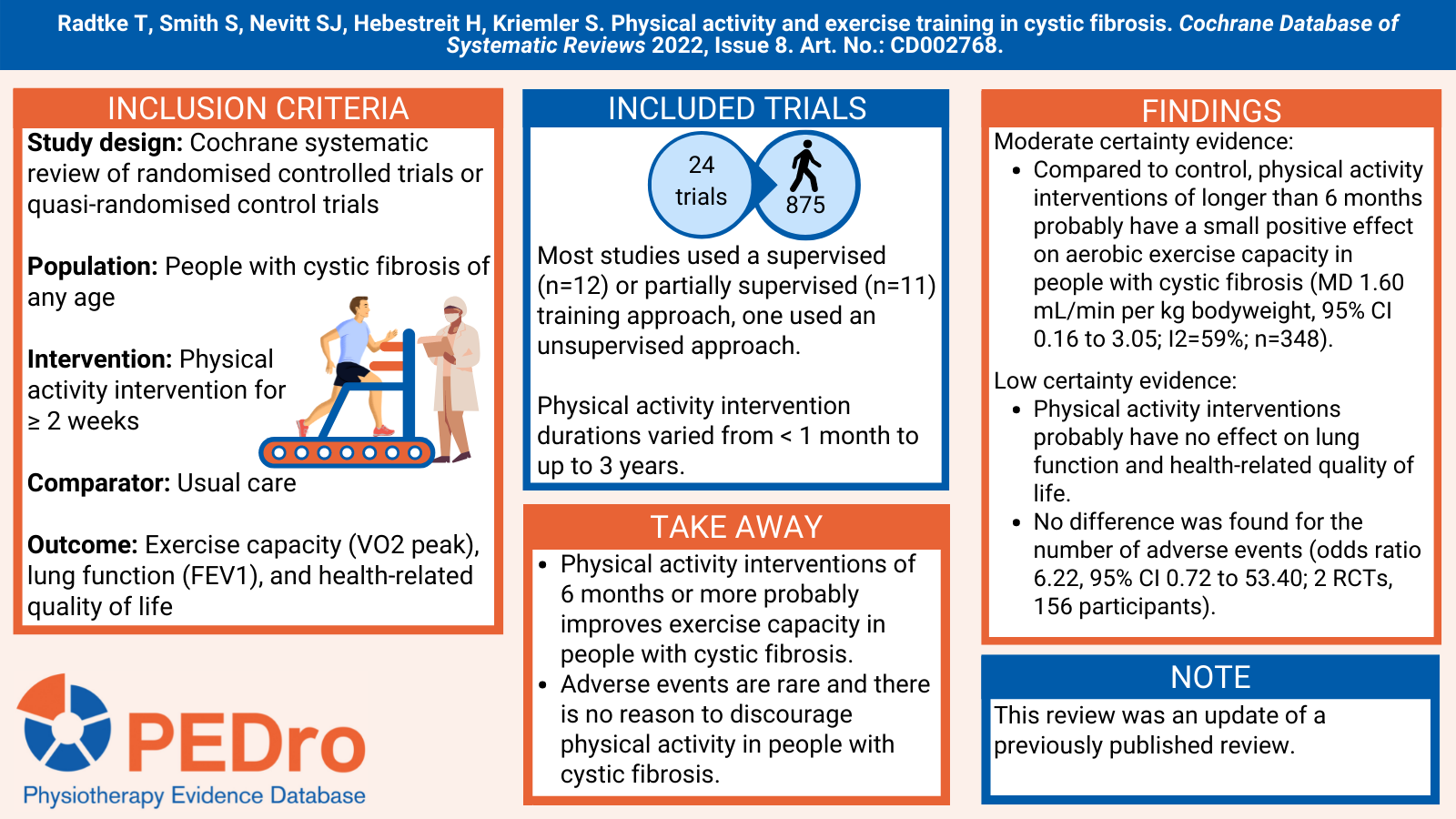
This Cochrane systematic review aimed to estimate the effects of physical activity on exercise capacity, lung function and health-related quality of life in people with cystic fibrosis. This review was an update of a previously published review.
This was a Cochrane systematic review of randomised controlled trials (RCTs) or quasi-randomised controlled trials. Relevant trials were identified from three trial registries. Trials were included if they included people with cystic fibrosis (of any age) who underwent any type of physical activity intervention compared to usual care (no physical activity intervention). Interventions needed to be two weeks or more in duration. The primary outcomes were exercise capacity (VO2 peak), lung function (FEV1), and health-related quality of life (using generic or disease-specific instruments).
Two review authors independently assessed studies for inclusion, extracted data, and undertook the assessment of risk of bias of included studies. Risk of bias was evaluated using the Cochrane risk of bias tool. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
There were 24 parallel RCTs included in the review (875 participants). Trial size varied from 9 participants to 117 participants and included a mix of adults, children, and adolescents. 12 studies used a supervised training approach, 11 used a partially supervised approach and one study used an unsupervised approach. Physical intervention durations varied from less than a month to up to 3 years.
Compared to no physical activity intervention (usual care), there was moderate certainty evidence that physical activity interventions of longer than 6 months probably have a small positive effect on aerobic exercise capacity in people with cystic fibrosis (MD 1.60 mL/min per kg bodyweight, 95% CI 0.16 to 3.05; I2=59%; n=348). There was low certainty evidence that physical activity interventions probably have no effect on lung function and health-related quality of life. No difference between groups was found for the number of adverse events over six months (odds ratio 6.22, 95% CI 0.72 to 53.40; 2 RCTs, 156 participants; low-certainty evidence).
Physical activity interventions of 6 months or more probably improves exercise capacity in people with cystic fibrosis. Adverse events are rare and there is no reason to discourage physical activity in people with cystic fibrosis.
Radtke T, Smith S, Nevitt SJ, Hebestreit H, Kriemler S. Physical activity and exercise training in cystic fibrosis. Cochrane Database of Systematic Reviews 2022, Issue 8. Art. No.: CD002768.
Psychosocial Interventions for the Treatment of Functional Abdominal Pain Disorders in Children: A Systematic Review and Meta-analysis
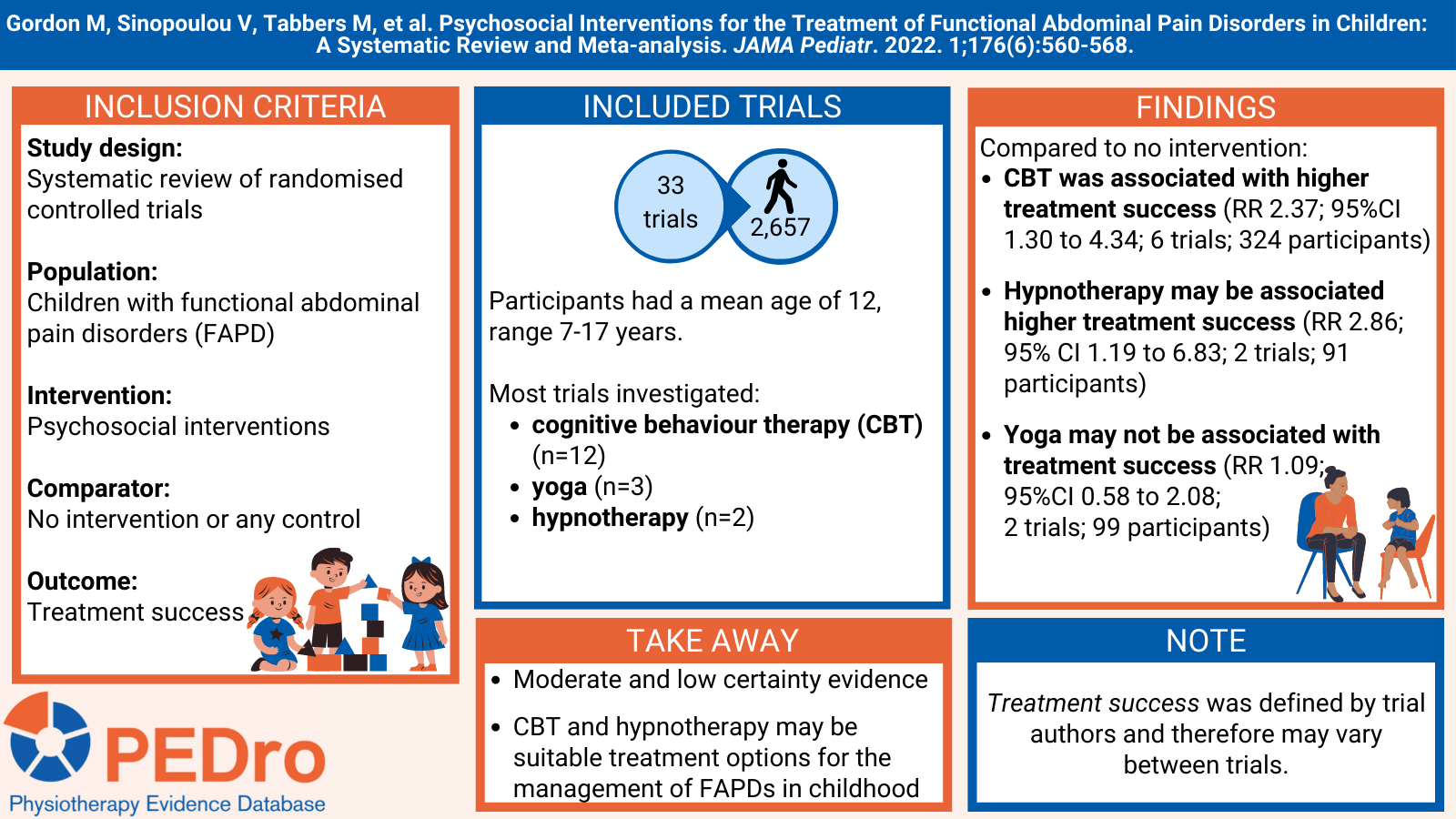
Functional abdominal pain disorders (FAPDs) can be divided into four subcategories (functional dyspepsia, irritable bowel syndrome, abdominal migraine and functional abdominal pain not otherwise specified). These painful conditions can severely affect the quality of life of children and their families, including reduced school/work attendance and performance. The management of FAPD can be time-consuming and financially costly for families and health care teams, with many children continuing to present symptoms as adults.
This systematic review aimed to estimate the effects of psychosocial interventions compared to no intervention or any control on outcomes treatment success, pain frequency, pain intensity, and withdrawal owing to adverse events in children (aged 4-18 years) with FAPD.
This systematic review registered their study protocol before data collection. Sensitive searches performed in five databases (including PubMed and the Cochrane Library) and three trial registries were used to identify randomised controlled trials (RCTs) published in any language. The review included participants who were children (aged 4-18 years) diagnosed with a FAPD defined by the Rome or similar criteria. Psychosocial interventions included cognitive behavioural therapy (CBT), yoga, hypnotherapy, educational support, gut-directed hypnotherapy, guided imagery, and relaxation. The comparators were no intervention or any control. The primary outcomes were treatment success, pain frequency, pain intensity, and withdrawal owing to adverse event.
Two independent reviewers selected trials for inclusion, evaluated risk of bias and extracted data. Any disagreements were resolved by consensus discussions or by a third reviewer. Trial risk of bias was evaluated using the Cochrane risk of bias tool and certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. Meta-analysis was used to pool the included trials to calculate risk ratio (RR) with corresponding 95% Confidence Intervals (CIs) for dichotomous data.
33 trials (2657 children) were included in the review. Participants had a mean [range] age of 12 [7-17] years and were predominately female (67.3%). CBT was the most investigated intervention compared to no intervention (n=12), followed by yoga (n=3) and hypnotherapy (n=2). The remaining trials (n=16) compared a psychosocial intervention with another active intervention.
Compared to no intervention, there was moderate certainty evidence that CBT was associated with higher treatment success (RR 2.37 (95%CI 1.30 to 4.34; number needed to treat [NNT] = 5; 6 trials; 324 participants); low certainty evidence that there may be no difference in treatment success with yoga (RR 1.09 (95%CI 0.58 to 2.08; 2 trials; 99 participants); and low certainty evidence that hypnotherapy may lead to higher treatment success (RR 2.86 (95% CI 1.19 to 6.83; NNT=5; 2 trials; 91 participants).
CBT and hypnotherapy were associated with higher treatment success compared to no intervention for the management of FAPD, whereas yoga was not. CBT and hypnotherapy may be suitable treatment options for the management of FAPDs in childhood.
Gordon M, Sinopoulou V, Tabbers M, et al. Psychosocial Interventions for the Treatment of Functional Abdominal Pain Disorders in Children: A Systematic Review and Meta-analysis. JAMA Pediatr. 2022. 1;176(6):560-568.
Read more on PEDro.
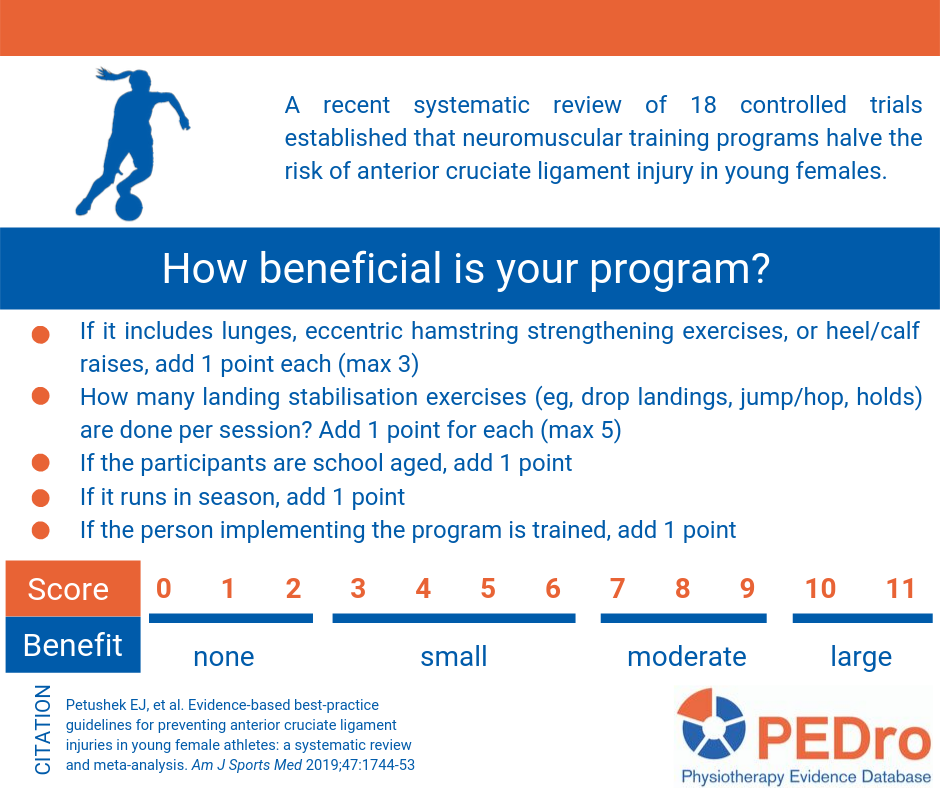
Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes
This systematic review compared neuromuscular training to any other intervention for preventing anterior cruciate injury in female athletes. Women were the focus of this evaluation because they are about three times more likely than men to injure their anterior cruciate ligament. The primary outcome was the number of anterior cruciate ligament injuries, but a precise definition of what was considered an anterior cruciate ligament injury was not provided. Meta-analysis was used to compare neuromuscular training to control conditions. In addition to determining the effectiveness of neuromuscular training, this review aimed to identify the common and effective components of anterior cruciate ligament neuromuscular training programs using meta-regression.
Prospective controlled trials were identified using sensitive searches in two databases (PubMed/Medline and CINAHL Plus). The PEDro scale was used to evaluate the risk of bias of the included trials. The review included 18 articles reporting the results for 20 trials (26,925 participants), 11 randomised controlled trials and nine non-randomised controlled trials. The mean PEDro score was 5.5 out of 10 (standard deviation 2.3). The average training dose was 57 sessions over 18.2 hours (or 24 minutes/session for 2.5 sessions/week). All neuromuscular training programs included instruction on proper program implementation for those carrying out the training. The included trials were conducted in soccer (n=7), handball (n=5), basketball (n=3), floorball (n=1) and mixed (n=4) sports in school (n=10), professional (5 trials), university (3 trials) and mixed-level (2 trials) athletes.
Compared to control interventions, neuromuscular training reduced the risk of anterior cruciate ligament injury from 1 in 54 to 1 in 111 (odds ratio 0.51; 95% confidence interval (CI) 0.37 to 0.69). Unfortunately the outcomes were not reported relative to exposure. Meta-regression indicated that the dose of neuromuscular training did not impact on injury risk, but the timing of training may be important. Neuromuscular training conducted only in the pre-season did not reduce the risk of anterior cruciate ligament injury (OR 0.59, 95% CI 0.16 to 2.15), while in-season only or combined pre-season and in-season training did reduce the risk of injury (OR 0.50, 95% CI 0.36 to 0.70). Programs targeting school-aged athletes had a larger effect (OR 0.38, 95% CI 0.24 to 0.60) than in older athletes (OR 0.65, 95% CI 0.48 to 0.89). Programs that contained knee stabilisation during landing and lower limb strengthening exercises were more effective than programs that did not contain these exercises. Programs that included balance, core-strengthening, stretching, or agility exercises were no more effective than programs that did not incorporate these components.
The review concluded that neuromuscular training reduces anterior cruciate ligament injury in female athletes. Data from the meta-regression were used to produce a best-practice checklist that can be used to evaluate neuromuscular training programs.
Petushek EJ, et al. Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes: a systematic review and meta-analysis. Am J Sports Med 2019;47(7):1744-53
Read more on PEDro.
Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions
The aim of this systematic review was to evaluate the effectiveness of scoliosis-specific exercises compared with other non-surgical interventions for adolescent with idiopathic scoliosis. Studies were eligible if they were randomised controlled trials evaluating scoliosis-specific exercises in participants with idiopathic scoliosis (defined as a primary Cobb angle of at least 10 degrees) and aged between 10 years and skeletal maturity. Scoliosis-specific exercises were defined ‘specific movements performed with a therapeutic aim of reducing the deformity.’ Comparators were non-surgical interventions, including bracing, electrical stimulation, manual therapy, generalised exercise, sports, active recreational activities, advice or waiting list. Primary outcomes were Cobb angle (in degrees) and angle of trunk rotation.
The review identified 9 studies (480 participants) that were conducted in Egypt, Brazil, Italy, Turkey, Korea, China, and Canada. There was variability in terms of the exercise parameters prescribed across studies. Treatment duration ranged from 3 weeks to 42 months.
Compared to general exercise or standard care, there was very low quality evidence that scoliosis-specific exercises reduced the thoracic Cobb angle (3 studies, 125 participants, mean difference -7 degrees,95% confidence interval (CI) -9 to -5), lumbar Cobb angle (2 studies, 105 participants, mean difference -7 degrees, 95% CI -10 to -4), and main curve location (3 studies, 172 participants, mean difference -5 degrees, 95% CI -9 to -1). Compared to general exercises or standard care, there was very low quality evidence that scoliosis-specific exercises did not reduce the angle of trunk rotation (1 study, 25 participants, mean difference -1 degrees,95% CI -3 to 5).
Very low quality evidence supports the use of scoliosis-specific exercise rather than standard care or other types of exercise for patients with adolescent idiopathic scoliosis to reduce spinal curvature. Large-scale and rigorous randomised controlled trials are required to evaluate the effectiveness and cost-effectiveness of scoliosis-specific exercise.
Thompson JY, et al. Effectiveness of scoliosis-specific exercises for adolescent idiopathic scoliosis compared with other non-surgical interventions: a systematic review and meta-analysis. Physiotherapy;105(2):214-34
The Effectiveness of Physical Therapy Interventions for Athletes Post-Concussion
This systematic review aimed to investigate the effects of physical therapy interventions compared to alternative treatments in adolescent and young adult athletes post-concussion.
Articles were included if they were randomized controlled-trials, had participants who were athletes under the age of thirty who had an acute or chronic sport-related concussion, and the intervention was physical therapy, including aerobic and multimodal interventions. Six databases were searched between March 2021 and January 2022. The PEDro scale was used to assess methodological quality of included trials to indicate high (>5/10), moderate (5/10) and low (<5/10) quality.
Eight articles were included in the review. Four assessed aerobic intervention and four assessed multimodal intervention. Multimodal treatment included individualised exercise progression, early intervention, cervical spine and vestibular rehabilitation, asymptomatic exercise and visualisation and imagery. Control treatment included stretching, education, subtherapeutic exercise, range of motion exercise, visualisation, rest and delayed intervention.
The outcome measures included the days from injury to recovery, PCSS, PCSI, Health Related Quality of Life, Beck Depression Inventory for Youth, Pediatric Quality of Life Multidimensional Fatigue Scale, the BESS, ImPACT, time to return to play, health and demographic questionnaires, Borg CR10, Rate of Perceived Exertion (RPE), and Post Ride Symptom Change Rating. The control groups either participated in education, rest, sub-therapeutic exercise, placebo, or sham treatment. None of the studies demonstrated any significant adverse effects from early physical activity and physical therapy intervention.
375 athletes (163 females and 212 males) participated in the eight studies with ages ranging from 11.2 to 21.2 years. The severity of symptoms ranged from acute post-concussion symptoms to chronic post-concussion symptoms. One article did not indicate the severity of concussion. Participants had either one concussion or a recurrence of concussions. Two articles did not indicate the occurrence of concussion.
Five of the eight articles were of a higher quality relating to risk of bias compared to the other three included articles, with scores ranging from a 5 to a 10 out of 10 points although there is no indication that the assessor had undertaken PEDro reviewer training.
Three of the five higher-quality articles found significant improvements in the treatment groups compared to the control groups with reduction in symptoms and time to recovery. All articles demonstrated improved symptoms with time and no notable adverse effects were reported with early physical activity and therapy. Due to the variability in the types of intervention utilised and the subjects on whom the interventions and controls were performed, the study was unable to determine the optimal treatment intervention.
This systematic review suggests that aerobic exercise or multi-modal interventions may lead to quicker recovery and return to sport in adolescent and young adult athletes with post-concussive symptoms when compared to traditional treatments such as physical and cognitive rest.

Art K, Ridenour C, Durbin S, Bauer M, Hassen-Miller A. The Effectiveness of Physical Therapy Interventions for Athletes Post-Concussion: A Systematic Review. Int J Sports Phys Ther. 2023 Feb 1;18(1):26-38.