Return to all evidence summaries
Sports
Sports includes papers which specifically mention sports injuries as well as conditions which commonly affect sports people (eg, ligament repairs).
The most recently synthesised review is at the top of the list.
- Do exercise-based prevention programmes reduce non-contact musculoskeletal injuries in football (soccer)?
- Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes
- Treatment and prevention of acute and recurrent ankle sprain
- Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players
- The Effectiveness of Physical Therapy Interventions for Athletes Post-Concussion
Do exercise-based prevention programmes reduce non-contact musculoskeletal injuries in football (soccer)?
Football (soccer) is a popular sport world-wide. Despite the health benefits of playing football, non-contact musculoskeletal injuries (eg, hamstring strain) are relatively common. Exercise-based programs have been developed to prevent injury, but previous evaluations have not differentiated between contact and non-contact injuries. This systematic review aimed to estimate the effects of exercise-based programs compared to control to prevent non-contact musculoskeletal injuries in football players.
Guided by a prospectively registered protocol, sensitive searches of six databases (including Medline, Embase and PEDro), three clinical trial registries and citation tracking were performed to identify randomised controlled trials evaluating exercise-based injury prevention programs. The participants were football players aged 13 years and older. The intervention was any exercise therapy performed to develop function, skills or physical fitness. The comparator could be usual training or warmup, minimal intervention, education or no intervention. The primary outcome was the occurrence of any acute sudden onset musculoskeletal injury that occurred without physical contact with another player or object on the field. In addition to reporting the number of non-contact injuries, included trials needed to report the number of exposure hours for each group. Two reviewers independently selected trials and extracted data. Disagreements were resolved through discussion or arbitration by a third reviewer. Risk of bias was evaluated using the PEDro scale, with scores downloaded from the PEDro database and confirmed by one reviewer. Certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The number of non-contact injuries and exposure hours were used to calculate the injury incidence rate per 1,000 hours and the injury risk ratio. Meta-analysis was used to compute the pooled injury risk ratio and its 95% confidence interval (CI). One pre-planned subgroup analysis was undertaken based on exercise type: focused/unimodal (exercises chosen to train and protect a specific muscle or joint) vs. generalised/multimodal (exercises that targeted many body segments) on non-contact hamstring injuries.
10 trials (13,355 participants) were included in the meta-analyses. The trials were conducted in the United States, Norway, and the Netherlands (2 trials each) and in Germany, Japan, Nigeria and Sweden (1 trial each). Only male players were included in 6 trials and only female players in 4. Most trials (7) recruited youth players and all trials included amateur players. The duration of the exercise-based program ranged from 3 to 9 months. Focused exercise was used in 3 trials (Nordic Hamstring Exercise, Bounding Exercise Program) and generalised exercise in 7 (Prevent Injury and Enhance Performance Program, FIFA 11+, FIFA 11, Knäkontroll (neuromuscular training)). All interventions were applied at least twice a week to every training session.
Exercise-based programs reduce the risk of non-contact injuries by 23% compared to control, with an injury risk ratio of 0.77 (95% CI 0.61 to 0.97; 10 trials; 13,355 participants; low certainty). The sub-group analysis revealed that focused programs were not different from generalised programs for the prevention of non-contact hamstring injuries. The injury risk ratio was 0.65 (0.44 to 0.97; 3 trials; 1,238 participants; low certainty) for focused programs and 0.63 (0.19 to 2.12; 3 trials; 2,573 participants; very low certainty) for generalised programs.
Exercise-based prevention programs may reduce the risk of non-contact musculoskeletal injuries in football players. Hamstring-focused programs did not reduce hamstring injury any more than general programs.
Lemes IR, et al. Do exercise-based prevention programmes reduce non-contact musculoskeletal injuries in football (soccer)? A systematic review and meta-analysis with 13,355 athletes and more than 1 million exposure hours. Br J Sports Med 2021 May 17:Epub ahead of print
Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes
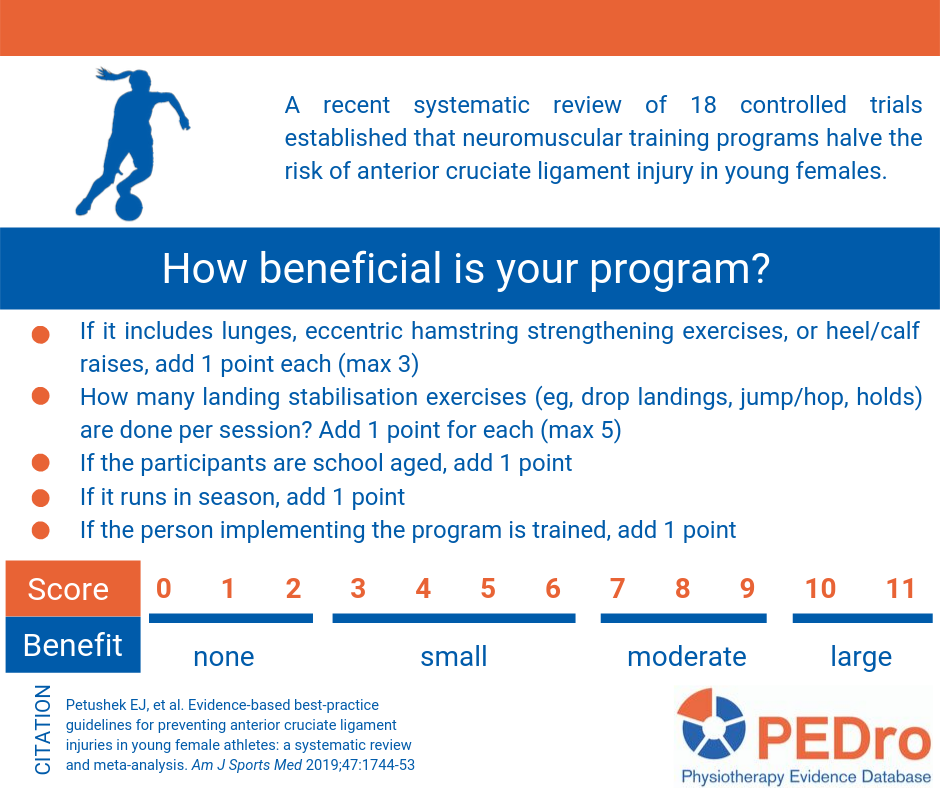
This systematic review compared neuromuscular training to any other intervention for preventing anterior cruciate injury in female athletes. Women were the focus of this evaluation because they are about three times more likely than men to injure their anterior cruciate ligament. The primary outcome was the number of anterior cruciate ligament injuries, but a precise definition of what was considered an anterior cruciate ligament injury was not provided. Meta-analysis was used to compare neuromuscular training to control conditions. In addition to determining the effectiveness of neuromuscular training, this review aimed to identify the common and effective components of anterior cruciate ligament neuromuscular training programs using meta-regression.
Prospective controlled trials were identified using sensitive searches in two databases (PubMed/Medline and CINAHL Plus). The PEDro scale was used to evaluate the risk of bias of the included trials. The review included 18 articles reporting the results for 20 trials (26,925 participants), 11 randomised controlled trials and nine non-randomised controlled trials. The mean PEDro score was 5.5 out of 10 (standard deviation 2.3). The average training dose was 57 sessions over 18.2 hours (or 24 minutes/session for 2.5 sessions/week). All neuromuscular training programs included instruction on proper program implementation for those carrying out the training. The included trials were conducted in soccer (n=7), handball (n=5), basketball (n=3), floorball (n=1) and mixed (n=4) sports in school (n=10), professional (5 trials), university (3 trials) and mixed-level (2 trials) athletes.
Compared to control interventions, neuromuscular training reduced the risk of anterior cruciate ligament injury from 1 in 54 to 1 in 111 (odds ratio 0.51; 95% confidence interval (CI) 0.37 to 0.69). Unfortunately the outcomes were not reported relative to exposure. Meta-regression indicated that the dose of neuromuscular training did not impact on injury risk, but the timing of training may be important. Neuromuscular training conducted only in the pre-season did not reduce the risk of anterior cruciate ligament injury (OR 0.59, 95% CI 0.16 to 2.15), while in-season only or combined pre-season and in-season training did reduce the risk of injury (OR 0.50, 95% CI 0.36 to 0.70). Programs targeting school-aged athletes had a larger effect (OR 0.38, 95% CI 0.24 to 0.60) than in older athletes (OR 0.65, 95% CI 0.48 to 0.89). Programs that contained knee stabilisation during landing and lower limb strengthening exercises were more effective than programs that did not contain these exercises. Programs that included balance, core-strengthening, stretching, or agility exercises were no more effective than programs that did not incorporate these components.
The review concluded that neuromuscular training reduces anterior cruciate ligament injury in female athletes. Data from the meta-regression were used to produce a best-practice checklist that can be used to evaluate neuromuscular training programs.
Petushek EJ, et al. Evidence-based best-practice guidelines for preventing anterior cruciate ligament injuries in young female athletes: a systematic review and meta-analysis. Am J Sports Med 2019;47(7):1744-53
Read more on PEDro.
Treatment and prevention of acute and recurrent ankle sprain
This study is an overview of intervention systematic reviews. The authors included 46 systematic reviews evaluating treatment and preventive strategies for acute ankle sprain and chronic ankle instability. The reviews included provided data from 309 individual studies. The primary outcomes were injury or re-injury incidence and function. The secondary outcomes were pain, strength, range of motion, proprioception and muscle activity in the ankle joint, and performance measures (i.e., biomechanical analyses of static or dynamic postural control, gait or jumping or landing tasks). The quality of the reviews was assessed using the AMSTAR tool and had a mean score of 6.5 out of 11. There is consistent evidence for exercise therapy and external supports (e.g., bracing, taping) for preventing ankle re-injury incidence (odds ratio 0.59, 95% confidence internal (CI) 0.51 to 0.68; odds ratio 0.38, 95% CI 0.30 to 0.47, respectively). For the treatment of acute ankle sprain, there is consistent evidence for non-steroidal anti-inflammatory drugs, early mobilisation, and exercise therapy for improving pain, swelling and function. There is limited evidence supporting the use of manual therapy for treating acute ankle sprain, although it does improve dorsiflexion range of motion. The efficacy of surgery and acupuncture are controversial and there is insufficient evidence to recommend ultrasound in the treatment of acute ankle sprains. There is a lack of evidence for orthotics or footwear for chronic ankle instability. The limitations of this review include the data extraction being conducted by only one reviewer and the high heterogeneity in the data presented in the included reviews.
Doherty C et al. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med 2017;51(2):113-25
Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players
In this new systematic review, the authors included 5 studies (4 cluster randomised controlled trials and 1 cohort study) that investigated injury prevention programs that included the Nordic Hamstring exercise on the hamstring injury rate in soccer players. Pooled data of 4,455 individuals included in the 5 studies were analysed. A total of 315,992 exposure hours and 166 hamstring injuries were collected from the included studies. The pooled results showed 51% overall injury reduction per 1,000 hours of exposure for to injury prevention programs that included the Nordic hamstring exercise compared to controls (injury risk ratio = 0.49; 95% confidence interval = 0.291 to 0.827; p = 0.008). A limitation of this review is that it was not possible to evaluate the isolated effect of Nordic Hamstring exercise because the injury prevention programs included a variety of other exercises. Another limitation is that cost effectiveness was not considered as an outcome in the review, even though economic data have been published.
Al Attar WS, et al. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: a systematic review and meta-analysis. Sports Med 2017;47(5):907-16.
The Effectiveness of Physical Therapy Interventions for Athletes Post-Concussion
This systematic review aimed to investigate the effects of physical therapy interventions compared to alternative treatments in adolescent and young adult athletes post-concussion.
Articles were included if they were randomized controlled-trials, had participants who were athletes under the age of thirty who had an acute or chronic sport-related concussion, and the intervention was physical therapy, including aerobic and multimodal interventions. Six databases were searched between March 2021 and January 2022. The PEDro scale was used to assess methodological quality of included trials to indicate high (>5/10), moderate (5/10) and low (<5/10) quality.
Eight articles were included in the review. Four assessed aerobic intervention and four assessed multimodal intervention. Multimodal treatment included individualised exercise progression, early intervention, cervical spine and vestibular rehabilitation, asymptomatic exercise and visualisation and imagery. Control treatment included stretching, education, subtherapeutic exercise, range of motion exercise, visualisation, rest and delayed intervention.
The outcome measures included the days from injury to recovery, PCSS, PCSI, Health Related Quality of Life, Beck Depression Inventory for Youth, Pediatric Quality of Life Multidimensional Fatigue Scale, the BESS, ImPACT, time to return to play, health and demographic questionnaires, Borg CR10, Rate of Perceived Exertion (RPE), and Post Ride Symptom Change Rating. The control groups either participated in education, rest, sub-therapeutic exercise, placebo, or sham treatment. None of the studies demonstrated any significant adverse effects from early physical activity and physical therapy intervention.
375 athletes (163 females and 212 males) participated in the eight studies with ages ranging from 11.2 to 21.2 years. The severity of symptoms ranged from acute post-concussion symptoms to chronic post-concussion symptoms. One article did not indicate the severity of concussion. Participants had either one concussion or a recurrence of concussions. Two articles did not indicate the occurrence of concussion.
Five of the eight articles were of a higher quality relating to risk of bias compared to the other three included articles, with scores ranging from a 5 to a 10 out of 10 points although there is no indication that the assessor had undertaken PEDro reviewer training.
Three of the five higher-quality articles found significant improvements in the treatment groups compared to the control groups with reduction in symptoms and time to recovery. All articles demonstrated improved symptoms with time and no notable adverse effects were reported with early physical activity and therapy. Due to the variability in the types of intervention utilised and the subjects on whom the interventions and controls were performed, the study was unable to determine the optimal treatment intervention.
This systematic review suggests that aerobic exercise or multi-modal interventions may lead to quicker recovery and return to sport in adolescent and young adult athletes with post-concussive symptoms when compared to traditional treatments such as physical and cognitive rest.
Art K, Ridenour C, Durbin S, Bauer M, Hassen-Miller A. The Effectiveness of Physical Therapy Interventions for Athletes Post-Concussion: A Systematic Review. Int J Sports Phys Ther. 2023 Feb 1;18(1):26-38. doi: 10.26603/001c.68071.
