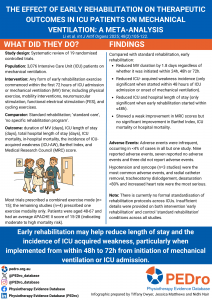
Patients in the intensive care unit (ICU) requiring mechanical ventilation often experience functional decline and complications attributable to reduced activity. Early rehabilitation could potentially improve functional outcomes and length of stay (LOS) in these patients, yet there is contention regarding the optimal time to commence early rehabilitation. This systematic review aimed to evaluate the clinical outcomes of early rehabilitation versus standard rehabilitation in mechanically ventilated patients in the ICU; and determine the optimal timing to implement early rehabilitation.
Methods
A prospectively registered systematic review and meta-analysis were conducted following PRISMA guidelines. Six databases were searched for randomised-controlled trials (RCTs), published in either English or Chinese, dating from inception to June, 2024. The databases included PubMed, Web of Science, Cochrane Library, CNKI, Wanfang Database and VIP Database. Reference lists from included studies were also reviewed. Eligible studies included patients on mechanical ventilation in the ICU who received early rehabilitation interventions (including physical exercise, mobility interventions, neuromuscular stimulation, functional electrical stimulation, or cycling exercises) versus those receiving standard rehabilitation. Two researchers independently conducted a literature search, preliminary screening and full text review of studies meeting the inclusion criteria, as well as independently extracting the data from included studies. Disagreements were resolved through discussion with a third reviewer.
Outcomes were the duration of mechanical ventilation, incidence of ICU-acquired weakness (ICU-AW), ICU and total hospital LOS, ICU and in-hospital mortality, Barthel index, and Medical Research Council (MRC) score. The early rehabilitation start time was categorised as within ≤24h, ≤48h or ≤72 hours from onset of ICU admission or initiation of mechanical ventilation for subgroup analysis. Quality of studies was assessed using the Cochrane Collaboration’s risk of bias tool. Certainty of evidence was not reported.
Results
19 studies (n= 3076 patients) were included in the final analysis, with 1541 patients receiving early rehabilitation. Included studies dated from 2009-2014. Trials were from China (n = 5), USA (n = 5) and remainder primarily from Europe. Patients were on average 48-67 years with an APACHE II score of 15-28 indicating moderate to high risk of mortality.
Interventions were a comprehensive exercise program (e.g. early mobilisation, in-bed cycling passive to active exercises, transfers) (15 studies), or single exercise modality (functional training) (4 studies). Early rehabilitation was commenced within 24 hours (4 studies), 48 hour (9 studies) or within 72 hours (6 studies).
Early rehabilitation reduced mechanical ventilation time by approximately 1.8 days (MD -1.80; 95% CI −2.64 to −0.96; 11 studies; 1047 participants) regardless of whether it was initiated within 24h (MD −2.51; 95% CI = −3.80, −0.43), 48h (MD −1.15; 95% CI = −2.10, −0.21), or 72h (MD −2.12; 95% CI = −4.42, −0.60) of ICU admission of onset of mechanical ventilation. Early rehabilitation also decreased the incidence of ICU-AW versus standard rehabilitation (RR=0.58; 95% CI =0.44 to 0.77; 6 studies; 641 participants); however this was only significant for the subgroup when early rehabilitation was started within ≤48h of ICU admission or onset of mechanical ventilation (RR 0.56; 95% CI= 0.39 to 0.81). Compared with standard rehabilitation, early rehabilitation decreased ICU length of stay (MD = -1.92 days, 95% CI -2.70 to -1.13; 17 studies; 2035 participants) which was consistent across all subgroups. Early rehabilitation also decreased total hospital length of stay (MD= -2.17 days; 95% CI -4.20 to -0.14; 14 studies; 2566 participants), however, this was also only significant for the subgroup when early rehabilitation started within ≤48h (MD= 3.71; 95% CI -7.13 to -0.29).
A weak association was found between early rehabilitation and improvement in MRC scores (MD= 4.12; 95% CI= 0.93, 7.31). There was no significant improvement in Barthel index of mechanical ventilation in patients who received early rehabilitation (MD= 8.37; 95% CI= -1.6, 18.35), and no improvement in either ICU mortality (RR= 0.76; 95% CI= 0.40 to 1.44; 6 studies; 489 participants) or in-hospital mortality (RR= 1.09; 95% CI = 0.86 to 1.38; 11 studies; 1780 participants).
Sixteen studies reported on adverse events; of those, 7 had 0 adverse events and 7 had fewer than 1%. One study reported 35 (3.6%) adverse events, 25 of which occurred in the treatment group. The most common AE was hypotension.
Conclusion
When compared with standard rehabilitation, early rehabilitation exercises may reduce mechanical ventilation time, the risk of ICU-acquired weakness, and decrease hospital and ICU length of stay in mechanically ventilated ICU patients. While there is currently no formal standardisation of rehabilitation protocols across ICUs, the optimal time to implement early rehabilitation may be within 48-72h or ICU admission or onset of mechanical ventilation, however further research is needed.
Li S, Xu X, Hu J, Wang Y. The effect of early rehabilitation on therapeutic outcomes in ICU patients on mechanical ventilation: A meta-analysis. Int J Artif Organs. 2025 Feb;48(2):105-122. doi: 10.1177/03913988241311816. Epub 2025 Jan 8. PMID: 39772978.